Medical tourism is becoming increasingly popular. Many patients from the United Kingdom go abroad for ophthalmic procedures. Complications may arise when back in the UK and are treated for free under the NHS. Currently NHS finances are becoming increasingly tight and these patients will add extra strain. We report a series of five cases describing complications and outcomes of three laser-assisted-in-situ-keratomileusis (LASIK) procedures, one phakic intraocular lens implant and one iris colour implant carried out abroad treated by one NHS consultant.
Cases 1, 2 and 3 were patients who travelled to India for LASIK procedures which were complicated by bilateral diffuse lamellar keratitis, sub-epithelial scarring, and flap malposition respectively. Case 4 had bilateral phakic intracocular lens implant and developed endophthalmitis. Case 5 was a gentleman who developed chronic anterior uveitis following bilateral iris colour implants in Panama City.
Front line ophthalmologists must be aware of complications of patients who have travelled abroad for medical treatments. Some of these are procedures which may not be offered on the NHS. The excess cost to the NHS for these five cases alone is estimated to be at least £11,587.
Background
Medical tourism is becoming increasingly popular, with 63,000 UK residents travelling abroad for treatment in 2010.1 The exact number seeking ophthalmology treatment is not known.
Common procedures include refractive surgery not available on the NHS, such as laser-assisted-in-situ-keratomileusis (LASIK) and intraocular lens implantation. Reasons for going abroad include cost savings, limited access to specific treatments and long waiting times. The majority of the patients featured in this article had travelled to India for their medical treatment. LASIK in the United Kingdom is estimated to cost on average of £1,742 per eye2 but costs just 15% of this price in India at £246 per eye.3
Return flights to various parts of India cost roughly £6004 and therefore a patient wanting bilateral LASIK would pay three times the cost in the United Kingdom (£3,484) compared to in India (£1,092).
It however poses safety risks to patients including those associated with travelling soon after surgery, difficulty assessing the quality of care and problems with continuity of care.
Patients will usually seek NHS services for complications that have arisen. NHS finances are under increasing strain, with the NHS chief making an unprecedented announcement stating non-urgent operation times will be allowed to rise to keep other services functioning.5
We present five patients who returned with complications following procedures abroad seen by one consultant corneal surgeon over 10 years and estimate the extra cost to the NHS that these patients have cost.
Case reports
Case 1
A 34-year-old gentleman underwent bilateral LASIK in India, in 2011. He presented three weeks later with reduced visual acuities; 6/9 in the right and 6/24 in the left. Anterior segments showed fine granular glistening at the interface; worse in the left eye (figure 1). He was diagnosed with bilateral diffuse lamellar keratitis and treated with Predforte and Exocin. Post treatment visual acuity improved to 6/9 bilaterally.
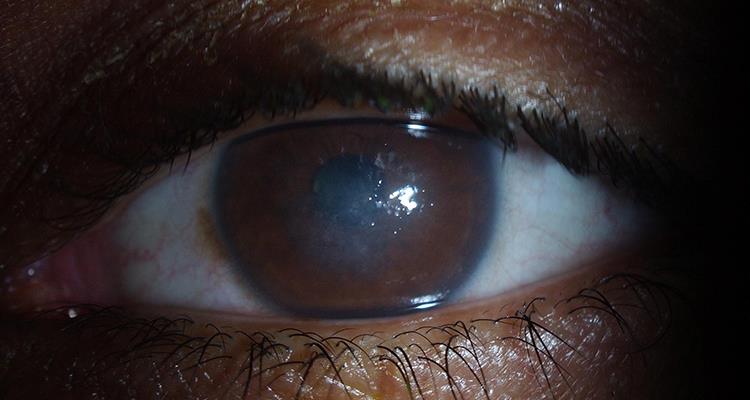
Figure 1: Bilateral diffuse lamellar keratitis
Case 2
A 41-year-old gentleman presented with 6/12 vision in the left eye eight months after undergoing bilateral LASIK procedures in India in March 2015. He was initially diagnosed with dendritic keratitis and treated with acyclovir ointment.
His vision further deteriorated to 6/60 and he was seen by the consultant corneal surgeon in January 2016. A dense sub-epithelial scar had developed on the visual axis with no corneal vascularisation (figure 2). Herpes simplex PCR was negative. The acyclovir ointment was changed to topical lubricants.

Figure 2: Corneal scarring of left eye
He subsequently developed superficial corneal vascularisation in two quadrants. A therapeutic ptosis was induced using botulinum toxin. He was considered for a graft, however, the corneal scar spontaneously improved and three years after his LASIK his vision is 6/9.
Case 3
A 51-year-old gentleman underwent bilateral LASIK in India in 2006. Four days post-procedure he presented with left eye visual acuity of 6/24. The cornea showed a fold in the flap obscuring the visual axis (figure 3). The patient required two revisions and repositioning of the flap. He achieved a best corrected vision with contact lenses of 6/4 bilaterally.

Figure 3: Flap striae within the cornea
Case 4 – Intraocular lens
A 35-year-old gentleman underwent simultaneous bilateral phakic posterior chamber intraocular lens implants in India in April 2015. Pre-procedure refraction was -7.00 DS bilaterally.
Four days post-procedure his left eye acuity was reduced to hand movements. Examination was suspicious of endophthalmitis and a vitreous tap cultured staphylococcus epidermidis. IOL explantation, vitrectomy and intravitreal antibiotics were given. His vision is now 6/60 and has developed cystoid macula oedema. It was decided after discussion with the patient that the right eye lens be left in situ currently and monitored for any signs of developing infection.
Case 5 – Iris colour implants
A 29-year-old man presented with low grade anterior uveitis one month after having bilateral iris colour change implants inserted in Panama City (figure 4). He was treated with topical steroids and warned that there were long term risks of further iritis, glaucoma and corneal decompensation. He has, however, insisted on keeping the implants in place. On regular review his pressures remain stable on twice daily steroids.
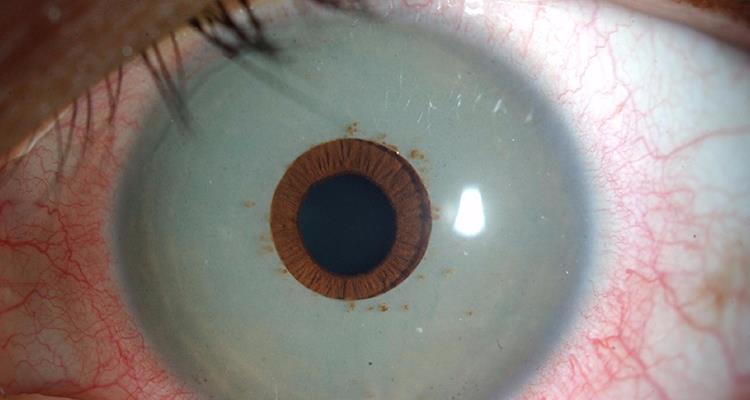
Figure 4: Bilateral pale blue iris colour inserts with pigment deposition. The pupillary margin and normal iris colour is visible beyond the implants in both eyes. There is also circumlimbal injection of the sclera bilaterally.
Discussion
The medical tourism industry is almost entirely unregulated. Medical tourists do not always inform their decision-making with hard information and do not consider all risks which has serious implications for informed consent.6 It can be extremely difficult for patients to access data regarding surgical outcome, for example UK ophthalmic consultant surgical outcomes are not freely available currently.
Researching a record of a surgeon operating in a foreign country’s private health sector is near impossible.
In 2008, the European Registry of Quality Outcomes for Cataract and Refractive Surgery (EUREQUO) formed a web-based registry aiming to improve treatment and standards of care for refractive surgery.
For LASIK surgery, a procedure only available privately in the UK, front line ophthalmologists must be aware of complications to manage patients effectively. Iris implants were developed for defects secondary to trauma or coloboma and even for these conditions doctors do not recommend implants due to complications described above.7 It is important for ophthalmologists to be aware of iris implants and to discourage patients from undergoing this procedure.8
These patients may represent the minority of patients having surgery overseas, however, they have added more than 50 outpatient appointments and four surgical procedures to a busy NHS trust. From the most recent pricing figures9 an initial consultation at a NHS hospital costs £113 and a follow up appointment costs £64.
A corneal operation is priced at £1,985, Botox at £1,100 and vitreoretinal operation at £1,408. The estimated cost to the NHS for these five patients is £11,583. The actual figure is likely to be higher as some notes were missing from the first case who is likely to have had more than two appointments, the cost of eye drops and intravitreal antibiotics has not been included and some appointments were emergencies which are tariffed at a higher rate.
Current NHS finances have come under increasing strain with non-urgent operation waiting times being allowed to rise to ensure other services continue to be delivered. As medical tourism becomes more common the impact on the NHS will continue to grow. There was recent debate regarding the role of the NHS to women who had been affected by the PIP (Poly Implant Prostheses) breast implants with some ministers lobbying that any costs incurred by the NHS for removal should be reimbursed.
The authors cannot find any conclusion to this argument which suggests they currently remain unresolved. Who the NHS would claim from in these procedures carried out abroad is under question. In addition, there may be a need for further national estimates of the cost to the NHS resulting from complications of procedures that patients have paid for whether that be abroad or in the UK to be able to budget for these patients.
We recommend all medical tourists take out comprehensive medical insurance and when deciding to choose surgery abroad seek advice from their doctor.
Ivan YM Yip and Balasubramaniam Ilango are consultant ophthalmologists at Wolverhampton Eye Infirmary, Edward WJ Pritchard at Royal Hallamshire Hospital, and Hanif Suleman at Burton Hospital.
References
1 Turner L. Beyond ‘medical tourism’: Canadian companies marketing medical travel. Global Health 2012;8: 16.
2 http://lasereyesurgery.cliniccompare.co.uk/the-average-cost-of-laser-eye-treatment?sid=10731177. Last accessed April 2017.
3 https://www.quora.com/Should-I-undergo-LASIK-eye-surgery-How-much-does-it-cost-in-India-Which-hospital-is-best-in-Hyderabad. Last accessed April 2017.
4 Opodo.co.uk. Last accessed April 2017.
5 NHS operations: Waiting times to rise in ‘trade-off’, boss says. BBC.co.uk. Last accessed April 2017.
6 Lunt N, Hardey M, Mannion R. Nip, tuck and click: medical tourism and the emergence of web-based health information. Open Med Inform J. 2010;4:1–11. doi: 10.2174/1874431101004010001.
7 Thiagalingam S, Tarongoy P, Hamrah P, et al. Complications of cosmetic iris implants. J Cataract Refract Surg 2008;34:1222- 4.
8 Shah RD, Randleman JB. New color iris implants. Ophthalmology. 2012;119(7):1495-1495.e1492.
9 2016/17 National Prices and National Tariff Workbook. Monitor. NHS England. Published 22 March 2017.