
My previous cases have focused on the use of the Topcon Myah in both the initial assessment of young myopic patients and in helping manage ocular surface disruption prior to introducing myopic management treatment with a contact lens option. Here, I present a new case where the initial discussion with the young myope and her parent suggested that the prescribing of myopia control spectacle lenses, the Hoya Miyosmart, would be a good idea.
Case Study
Initial findings
Fourteen-year-old female, LH, became aware of difficulties reading the classroom board upon returning to school after lockdown (figure 1). Her previous eye exam had been some 18 months. Points of relevance included:
- Mother is an astigmatic myope
- Last Rx (October 2019);
- R: -1.75 / -2.25 x 3 (6/6)
- L: -1.25 / -2.75 x 3 (6/6)
- New Rx (March 2021)
- R: -2.75 / -2.00 x 6 (6/6)
- L: -1.25 / -2.75 x 180 (6/6)
- LH very resistant to the idea of contact lenses
- Binocular status;
- Cover test; orthophoric at distance, compensated exophoria at near
- 0.50DS accommodative lag (by retinoscopy)
- Myah baseline data;
- Axial lengths (figure 2); R 26.35mm, L 26.20mm
- Keratoconus risk assessment (figure 3); negative
- Aberrometry (figure 4); R&L astigmatism, L greater high order aberration
Note how the axial length is already over 26mm, surprising for the low myopia; it was a shame there was no previous axial length data available. Having accurate data now will be essential as we attempt to manage the myopic progression, helping to see the impact upon progression rate and in predicting likely future growth.
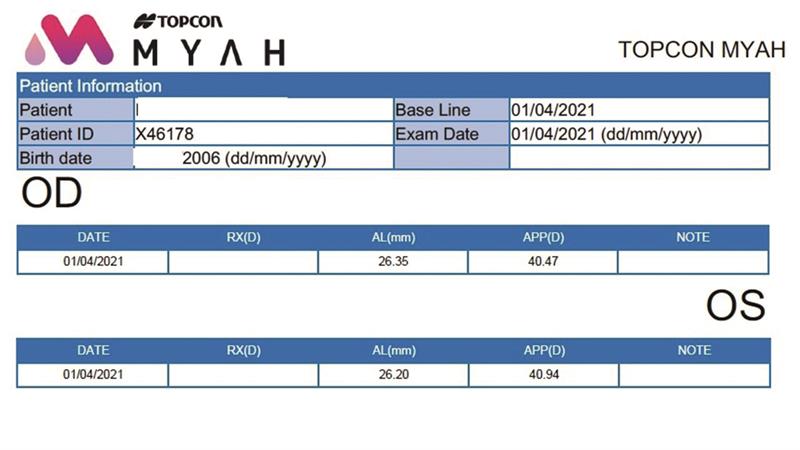 Figure 2
Figure 2
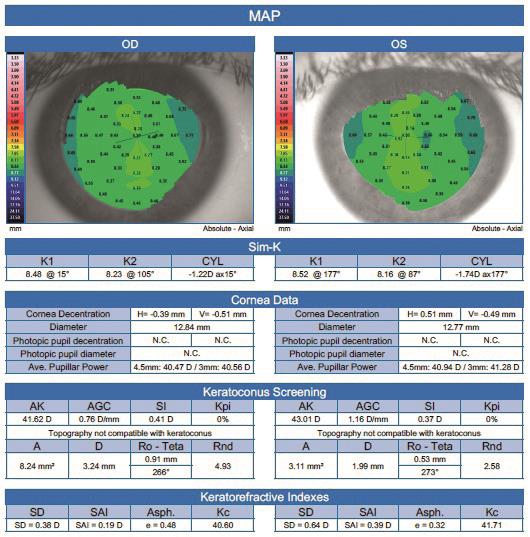 Figure 3
Figure 3
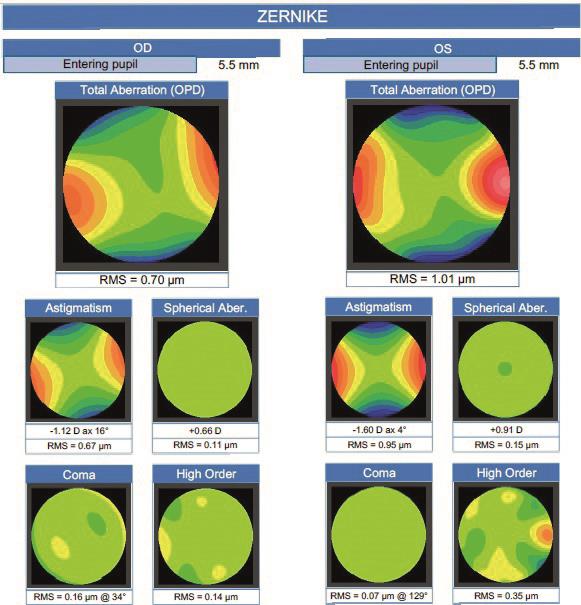 Figure 4
Figure 4
Patient discussion
The various management options were explained directly to LH with her mother listening on. It is essential always to engage the patient as number one if future compliance is to be assured. The level of cylinder ruled out both peripheral defocus contact lenses and orthokeratology, never mind LH’s existing resistance to a contact lens option. That said, the relatively high axial length meant that some growth control was worth attempting.
LH, her mother and me then agreed that, in this case, myopia control spectacle lenses would be worth trying. They had already read about the Hoya Miyosmart lenses, were impressed by the initial trial results showing significant myopia progression slow down, but I still took time explaining the concept and emphasised how the aim is to slow progression but not stop or reverse it. I found it useful to also recommend both the Hoya and the CooperVision websites for further information; the more aware the patient, the better the chances of success.
Our dispensing optician is accredited to dispense the Miyosmart so was able to advise on best frame and take accurate mono PDs and heights. LH was also impressed when shown a dummy lens when the concept of the ‘lenslets’ was explained.
Plan
We will review LH in six months time, during which our optician will always be at the end of a phone if LH has any concerns. Look out for results in a future feature.
* A video of our discussion can be accessed via the online version of this feature.
Sarah Farrant is a therapeutic optometrist with a specialist interest in dry eye disease and myopia management practising in Somerset, UK.