
A laudable trend in recent years has been the increased use of patients in CPD live events. While most of the facts and details heard during lectures and webinars might just as easily be learned from a good reference list and library, listening to the real-life experiences of patients and practitioners is what makes a good live education event so worthwhile.
An excellent example of this was the recent College of Optometrists webinar focusing on the latest developments in cataract and vitreoretinal surgery. Over 1,000 delegates tuned in to the online event to hear from, not only the always excellent consultant ophthalmologist Kam Balaggan, but also the three patients who had undergone the new treatments under discussion. Hearing the reactions of each of them, as they realised that they were watching a film of their own eye being operated on, was quite something. And, interesting as it was to hear about new surgical procedures, it was the descriptions from the patients of how their lives had changed since treatment and what they felt as the surgery was being carried out that will stay in the memory most. This approach to teaching is something Mr Balaggan feels strongly about, hence the main title of the session: ‘The patient as the teacher.’
Each patient had an interesting story to tell. The first told how surgery to remove his extensive vitreous floaters had changed his life, the second explained how sight loss due to an epiretinal membrane had been treated, while the third, who had the most significant history of sight loss, was able to describe his traumatic experience of sight loss due to subluxation of his intraocular lens.
Myodesopsia
Floaters are usually accepted as a sign of the normal ageing process affecting the eye and, unless there is a sudden change in size or nature, most are usually dismissed as something to ‘get on with’ and ‘get used to’. Whether a result of vitreous syneresis, a posterior vitreous detachment (PVD), or secondary to an underlying disease such as haemorrhagic floaters from retinopathy, calcium soaps from asteroid hyalosis (figure 1) or inflammatory changes from uveitis, the key thing is always to establish the likely cause and then to treat as appropriate.
For a surprisingly high number of people, as the number of floaters increases, vision can be adversely affected (especially contrast sensitivity), sometimes to a level where there is a significant impact on everyday life. At this point, the usual process of neuroadaptation is failing and the patient is said to have vision degrading myodesopsia (VDM) and should now be told about treatment options. To underline the significance of the problem, Mr Balaggan showed a snapshot of the very many online testimonials describing the trauma of VDM and the benefits of its treatment.

Perhaps most famous of these is the various videos posted by TV presenter Phillip Schofield who, until his successful vitrectomy procedure, was finding the shadowing caused by his many floaters was preventing him from carrying out his duties on ITV’s This Morning show (figure 2, right).
I am old enough to remember being told how complicated and potentially harmful a vitrectomy was, and so was used only when alternatives were exhausted. In recent years, however, improvements in surgical techniques have reached a point where a vitrectomy is a safe and effective management option for serious floater concerns.1 Paraphrasing floater expert Dr Jerrry Sebag, the man responsible for coining the term VDM, Mr Balaggan explained that vitrectomy ‘normalises vision and improves quality of life cost-effectively.’ And with the evolution of laser and pharmacological vitreolysis therapies on the horizon, vision-impacting floaters could soon be a thing of the past.
Indications for vitrectomy include the following:
- Chronic symptoms experienced for more than six months
- Age 45 to 50 years or more (though the presence of a PVD makes treatment of younger patients viable)
- PVD: though not essential, this reduces the risk of complications
We then heard from 53-year-old Dominic (figure 3, below), a moderate myope for whom floaters had become intolerable and preventing him from living his life as he would have liked to.
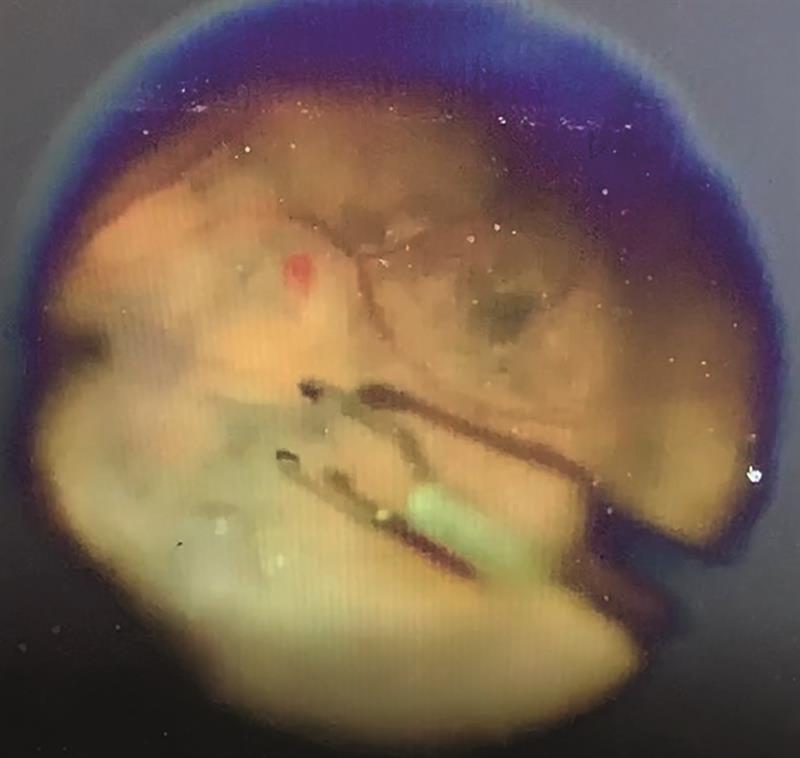
Mr Balaggan then outlined the procedure, which he performed in March 2020; a right, 25-gauge micro-incision, sutureless, vitrectomy. The 20 to 30 minute procedure is carried out under local anaesthetic and while the risks of blindness (<1 in 1,000) and retinal detachment (between 1 in 200 and 1 in 300) are small, subsequent cataract progression is guaranteed. We then were able to join Dominic in watching the procedure on-screen (figure 4).
Figure 4: (a) Introduction of ports; (b) PVD induction; (c) triamcinolone-assisted vitrectomy; (d) cryotherapy; (e) removal of ports

Despite the development of post-operative cataract, Dominic had been ‘delighted’ with the outcome and was awaiting cataract removal in the near future.
Epiretinal Membrane
Epiretinal membranes are common, with an 11.8% unilateral prevalence and bilateral of 2.4%. While the majority are asymptomatic and stable, contraction may lead to complications including retinal folding, macular thickening, vision loss, metamorphopsia, micropsia and monocular diplopia (figure 5, right; example of contraction of epiretinal membrane resulting in visual distortion). Visual distortion may be a reason for surgery, even if static acuity is still reasonable.
Andy had epiretinal membrane in his right eye, having lost sight in the left after an anterior ischaemic optic neuropathy, which was further complicated by the presence of a horseshoe tear.
He underwent a right 25-gauge microincision vitrectomy, epiretinal and internal limiting membrane peel (figure 6; left), cryotherapy, capsulotomy and gas injection to address these changes.
With 6/5 acuity restored, Andy was ‘delighted’.
Complex Subluxed Intraocular Lens
The final case for discussion was 74-year-old Leslie who had, among several other complications including pseudoexfoliation glaucoma, suffered an inferior subluxation of an IOL after it had been severely pitted during a YAG capsulotomy procedure. To correct the aphakia, the decision was made to use a new technique (Yamane method) whereby the replacement IOL would be intra-sclerally fixed (figure 7).
Figure 7: (a) The Yamane double-needle technique allows IOL positioning via haptics fed into tubes set in the sclera; (b) Mr Kam Balaggan successfully positions a replacement IOL in Leslie’s eye using the technique

Top Marks
Literally cutting-edge education combined with patient experiences. What could be better? College members can access materials produced by Mr Balaggan on the CoO website college-optometrists.org/my-college.
References
- Mason JO et al. Safety, efficacy, and quality of life following sutureless vitrectomy for symptomatic vitreous floaters. Retina. 2014 Jun;34(6):1055-61