
Case
MC, a sprightly lady in her early 70s, attended the practice for a sight test and a contact lens refit. She had been using single vision rigid gas permeable lenses for 40 years and was getting tired of using her over-readers daily. She also needed to use her spectacles more often and wanted to ‘try something new.’
Initial Presentation
Assessment confirmed her moderately myopic distance vision correction (approximately -4.50DS in either eye with minimal cylindrical correction) and a presbyopic add. After some discussion, we agreed that she might start off by trying some daily multifocal contact lenses. Prior to fitting, I discovered that she had some dry eye signs as follows;
- Low grade corneal ‘smile’ staining
- Reduced fluorescein break-up time of around 6 to 7 seconds (figure 1)
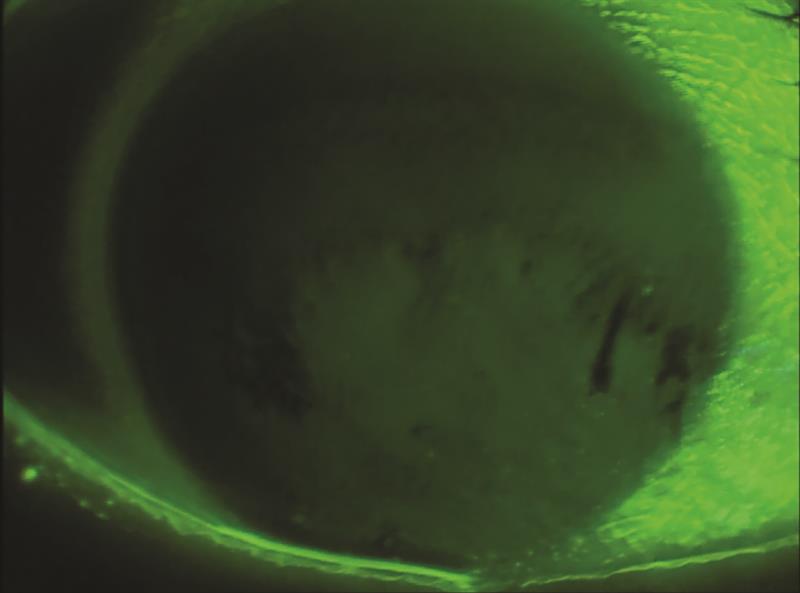 Figure 1
Figure 1
So, after discovering her best-vision sphere and eye dominance (left eye), and following the manufacturer’s fitting guide, I successfully fitted some daily disposable multifocal lenses as follows;
- RE: -4.00DS HIGH
- LE: -4.00DS MID
MC went away happy after an application and removal appointment with one of the clinical assistants and I arranged to see her in a week.
First Review
On review, MC ‘couldn’t get over how comfortable her lenses were compared to her old RGPs’ and ‘could definitely appreciate the reading improvement.’ However, she complained of intermittent blurring, worse in the evening, which took several blinks to clear before quickly blurring again. I suspected that her tear film was to blame. However, MC was convinced that ‘these are not the lenses for me.’
We chatted through the options, including trying a different pair of lenses and addressing the dry eye problems. She didn’t seem to grasp the possibility that her ‘dry eyes’ could be the cause her visual disturbances. ‘Surely, it must be the lenses?’ she asked.
So, I adjusted the lenses (according to the fitting guide), and sent her off with a modified Rx to boost her reading and a bottle of preservative free topical lubricant to try.
Second Review
A week later, MC reported the same problem with the lenses; intermittent blurring. So, I discussed the dry eye possibility again. She still didn’t seem to appreciate this as a possible cause, again citing the lenses as the problem. So again, after some debate, I tried a different brand of lenses. These were fitted and, after assessment of fit and vision, she was once again sent away to trial these.
Third Review
Around 5 days later and MC is back in my chair. ‘These lenses are really comfortable, but I still can’t read for very long’. I checked the acuity and fit, which were fine in the room (binocularly 6/6 and N6), took the lenses out and did a full slit lamp assessment. This revealed;
- mild-moderate ‘smile’ staining on her corneas
- a normal central tear prism
- some lid parallel conjunctival folds (LIPCOF)
- minor lid changes, including notching and telangiectasia
- (figure 2)
I got my MGD forceps out and gave her lids a good squeeze; et voila, grade 3 meibomian gland dysfunction (MGD) with thickened and waxy meibum expressed. ‘Here’s your problem’, I exclaimed.
So, MC went away with an eye mask to be heated in the microwave with instructions to use it for 10 minutes daily. This was further supported by some lid massage (I usually explain this by ‘think tired toddler’), lid hygiene instructions (plus wipes for her eyelids), a bottle of Omega Eye capsules (2000mg daily) and advice to use her topical lubricant (previously dispensed) at least four times a day or more if needed.
A phone call a week later revealed a significant improvement in symptoms. Things were not yet perfect, but much better than before and MC was enjoying much more stable vision. In hindsight, I should have tackled her dry eye at the start, but as we all know, hindsight is a wonderful thing!
Dr Tony Gibson PhD, BSc (Hons), FCOptom DipTP(IP), Prof Cert Glauc, Prof Cert Med Ret, is a practicing therapeutic optometrist and Director of Cooper & Leatherbarrow Ltd.