
In the first half of this two-part review, we looked at the attitudes, opinions, and understanding of parents regarding myopia and its management in their children. In brief, we saw that parents need to be made aware of the risks associated with myopia and that parents want eye care professionals (ECPs) to explain the available options for myopia management.1 This second half of the review presents the findings of a webinar survey that examined the current myopia management practices and views of ECPs.
Myopia is being increasingly recognised as a serious public health concern and is prompting greater discussion between researchers and ECPs at conferences and other events. So far, the conversation about myopia and its management has focused on presenting the findings of recent research; however, this research needs to be translated into clinical practice. Webinars (online training seminars) are one way to address this need for education and practical advice on how to select and manage myopic patients in practice. Webinars are not only a convenient way to provide this information to a large audience, but also allow for elements of dialogue, such as Q&As and other feedback. During recent webinars on the subject of integrating MiSight 1 day myopia control contact lenses into practice, individuals from eye care practices participated in a survey examining their current practice and views with respect to myopia management.2
Method
The webinar survey was offered to ECPs who wanted accreditation in order to use MiSight 1 day in practice. Seven webinar surveys were conducted among eye care practitioners from the UK and Ireland from August 2018 to January 2019.
Of the 1,367 ECPs in the webinar survey, most were ECPs, whereas 26 were non-ECP and therefore removed from the analysis. The ECPs included 1,139 optometrists, 164 contact lens opticians (CLOs), 37 trainee CLOs, and one ophthalmologist.
Results
An overwhelming majority of ECPs did not yet use any myopia management strategies with young myopic children. A total
of 877 ECPs were not using any strategy, 85 were using
orthokeratology, 81 were using centre-distance multifocal contact lenses, 48 were using bifocal or multifocal spectacles, and 24 were using some other strategy. However, 57% (682/1,203) of ECPs indicated that they had noticed an increase in the prevalence of myopia in children under 16 in their practice. Furthermore, most ECPs (77%) believed that fitting children with myopia control contact lenses carried less risk than the potential risks of future ocular pathology. Only 3% believed they carried more risk than the potential for future ocular pathology.
ECPs reported that, in their experience, parents were chiefly concerned that their child’s myopia would lead to an ‘increasing prescription and needing stronger glasses’ (75%) and ‘having to rely long-term on vision correction everyday’ (24%). Few ECPs reported that parents were concerned about an ‘increased risk of myopia-related ocular pathology in later life’ (0.4%) or ‘impact on future career options’ (0.2%). Likewise, few ECPs reported that parents were unconcerned about their child’s myopia (0.5%).
Almost half (48%, 618/1,274) of ECPs indicated that a myopia control intervention would need to demonstrate an average reduction in myopia progression of 25 to 50% before they would recommend it. A further 21% of ECPs would need an average reduction of ‘at least 25%’. The remaining ECPs selected more demanding requirements, with 29% requiring an average reduction of 51 to 75% and 2% requiring an average ‘over 75%’.
Approximately one-third (32%, 416/1,277) of ECPs reported that they believe children can be successfully fitted with contact lenses from the age of ‘six or seven’ years. Over half (53%) of ECPs selected an age of ‘eight or nine’, 12% selected age 10, 2% age 11, and 1% age ‘12 and above’.
A majority of ECPs believe that myopia management using contact lenses will become the standard of care for myopic children. Only 7% of ECPs disagreed with this, and 24% indicated that they did not know.
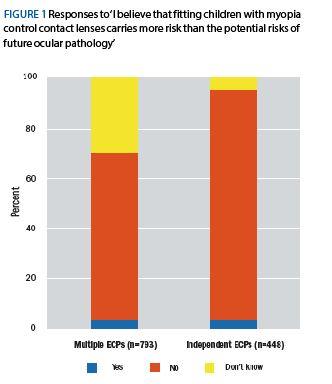 Figure 1: Responses to ‘I believe that fitting children with myopia control contact lenses carries more risk than the potential risks of future ocular pathology’
Figure 1: Responses to ‘I believe that fitting children with myopia control contact lenses carries more risk than the potential risks of future ocular pathology’
The proportion of response types for most questions appear to be similar between ECPs working in independent and multiple practices although independent ECPs might hold a greater belief that myopia control contact lenses carry less risk than allowing myopia to continue unabated and will become the standard of care (figure 1 and figure 2).
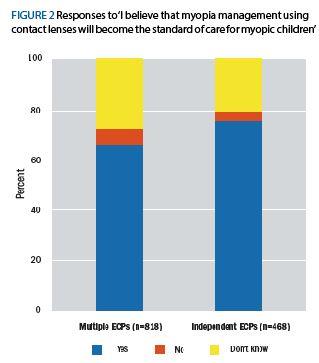 Figure 2: Responses to ‘I believe that myopia management using contact lenses will become the standard of care for myopic children’
Figure 2: Responses to ‘I believe that myopia management using contact lenses will become the standard of care for myopic children’
Discussion
The main findings of the webinar survey are:
i Many ECPs are not prescribing myopia management despite noticing an increased prevalence of myopia and their understanding of myopia-associated pathologies,
ii The experience of ECPs with respect to parents’ concerns is in agreement with parents’ lack of awareness of the risks associated with myopia
iii Most ECPs would require that a myopia control intervention demonstrate an average reduction in myopia progression of between 25 to 50%
iv Most ECPs believe children can successfully wear contact lenses from the age of eight or nine.
Surveys suggest that the views of ECPs might be moving in favour of fitting younger children. A survey conducted in 2013 by the College of Optometrists found that most ECPs believed ‘10 to 12 years’ to be the appropriate age for introducing children to soft contact lenses.3 In contrast, most respondents of the webinar survey selected ‘eight or nine years’ as the age at which children can be successfully fitted with contact lenses. The College survey also observed that optometrists were more likely to fit contact lenses to children of younger ages than they had been during the previous five years.3 Optometrists selected young patients for contact lens wear based on factors such as the child’s motivation, maturity, and hygiene practices rather than age.
The findings of the webinar survey are consistent with those of Wolffsohn et al (2016) who conducted an internet-based survey of 971 ECPs from around the world.4 Wolffsohn et al reported that a vast majority of ECPs (68%) are still prescribing single vision corrections to young myopic patients. This lack of myopia management is in spite of ECPs’ high levels of concern about the increasing prevalence of paediatric myopia and relative confidence in the effectiveness of myopia control strategies. The main reasons ECPs gave to explain why they were unwilling to prescribe alternatives to single vision corrections were: increased expense (36%), insufficient information (33%), and the unpredictability of clinical outcomes (28%).
Myopia management
Eye care professionals may wish to build their confidence with myopia management by fitting myopia control contact lenses to existing myopic, contact lens wearing teenagers. Figure 3 provides an approach to the management of children in practice based on their risk of myopia.
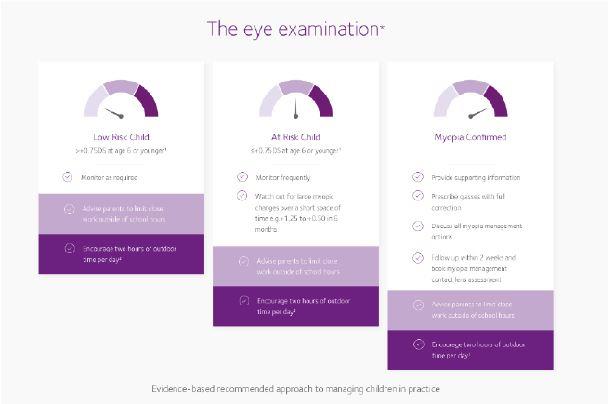 Figure 3: Managing myopia in practice [Taken from: CLEERE Study Group Early Childhood Refractive Error and Parental History of Myopia as Predictors of Myopia. Invest Ophthalmol Vis Sci. 2010 Jan; 51(1): 115–121]
Figure 3: Managing myopia in practice [Taken from: CLEERE Study Group Early Childhood Refractive Error and Parental History of Myopia as Predictors of Myopia. Invest Ophthalmol Vis Sci. 2010 Jan; 51(1): 115–121]
MiSight 1 day
MiSight 1 day is the first soft contact lens proven to slow the progression of myopia in children. This dual focus, soft, daily disposable contact lens not only corrects the child’s myopia but can also help to slow the progression of myopia by creating myopic defocus over the entire retina. MiSight 1 day has proven its effectiveness as a myopia control contact lens during a three-year, randomised clinical trial; compared to a control group (Proclear 1 day), MiSight 1 day wearers demonstrated a 59% reduction in the rate of myopia progression as measured by spherical equivalent refractive error. Similarly, the wearers demonstrated a 52% reduction in axial growth. These three-year efficacy data have just been published in Optometry and Vision Science,6 and five-year data – presented at the BCLA conference in June by Paul Chamberlain – continue to show excellent results, with both groups of children now wearing the MiSight 1 day lens.7 In addition, 95% of parents reported that their children were happy with the comfort of the myopia control lens.
Furthermore, 90% of children preferred their MiSight 1 day lenses to wearing their spectacles, and 90% of children agreed the lens provided clear vision for a range of daily activities.
Conclusion
Recent surveys of parents and ECPs confirm several findings from the few previous surveys that examined views on myopia management. Most parents do not consider myopia as a health risk since they do not realise that myopia is associated with other eye health problems in later life. Instead, parents are mostly concerned about the effect of myopia on prescription strength. Parents are also largely unaware of the various strategies used to slow the progression of myopia, but they are keen to hear about all available options. Many parents are initially worried that contact lenses are too risky for children, although ECPs may help alleviate concerns by recommending contact lenses and explaining the potential for myopia control.
The views of ECPs from the UK on contact lenses seem to be moving in favour of fitting younger children. This may be because ECPs are noticing a concerning increase in the prevalence of paediatric myopia; furthermore, practitioners are confident in the effectiveness of myopia control contact lenses. However, many UK ECPs do not use any myopia management strategy and are likely to be prescribing single vision corrections to their young myopic patients. One reason for this may be that ECPs need to develop their knowledge, communication skills and confidence in myopia management.
The survey findings imply that ECPs and parents need education on the topic of myopia management. Many ECPs are interested in myopia management and MiSight 1 day contact lenses, but ECPs and their support staff need education to build their confidence. A number of sources of information are available, including BCLA courses, journal articles, and conferences. Similarly, parents want to make informed decisions but need ECPs to provide them with well-written, evidence-based resources that explain myopia, its development and the available management options. Now is the time to raise awareness of myopia among ECPs and the public to ensure that all myopic children can benefit from myopia management at the earliest opportunity.
Australian Seminar Survey
A poll of 443 Australian eye care professionals was conducted at a series of myopia management seminars in March of 2019.5 Most ECPs (89%) were currently prescribing myopia control strategies, including progressive spectacles (70% of ECPs) and soft multifocal or bifocal contact lenses (60%). However, soft contact lenses were the main prescription for just 14% of ECPs, whereas progressive spectacles were the main prescription for 40% of ECPs.
Nearly all (97%) of the ECPs agreed that, when examining a new or existing young myope, optometrists should be expected to explain the risks of myopia and the possible management options with the child’s parent or parents. Among those who were not practising myopia management, ECPs most commonly cited ‘lack of specialist equipment’ (34%) and not having ‘enough knowledge’ (32%) as the main reasons for not doing so.
Optician will be publishing a review of the latest MiSight research data in the next Contact Lens Monthly
Elizabeth Lumb is EMEA Head of Professional Services for MiSight 1 day at CooperVision where Anna Sulley is Director Global Medical Affairs.
Acknowledgement
Thanks to Nathan Greenaway at Visioncare Research Ltd for his help in preparing these articles.
References
1 CooperVision Data on file. UK YouGov Consumer Study – March2019.
2 CooperVision Data on file 2019. UK ECP webinar.
3 The College of Optometrists. UK contact lens practice for children and young people survey. https://www.college-optometrists.org/the-college/research/research-projects/contact-lens-practice-children.html.
4 Wolffsohn JS, Calossi A, Cho P, Gifford K, Jones L, Li M, Lipener C, Logan NS, Malet F, Matos S, Meijome JM. Global trends in myopia management attitudes and strategies in clinical practice. Cont Lens Anterior Eye. 2016;39:106-16.
5 Coopervision Data on file 2019. Australian ECP seminar.
6 Chamberlain P, González-Méijome JM, Logan NS, Ngo C, Jones D, Young G. A Three-Year Randomized Clinical Trial of MiSight 1 day Lenses for Myopia Control. Optom Vis Sci 2019; Vol 96(8). Article in Press.
7 Chamberlain P, Logan N, Jones D, Gonzalez-Meijome J, Saw S-M, Young G. Clinical evaluation of a dual-focus myopia control 1 day soft contact lens: 5-year results (2019 BCLA Clinical Conference & Exhibition).