Cataract surgery is the most commonly performed surgical procedure in the world, with an estimated 19 million operations performed annually. According to estimates from the World Health Organization, this number will increase to 32 million by the year 2020 as the over-65 population doubles worldwide. In England and Wales approximately 160,000 cataract procedures are performed each year, with an annual increase of about 7%. There is an estimated cataract backlog of 2.4 million people with visual impairment due to cataract with 1.1 million new cases expected over five years.
Cataract surgery now accounts for more than half the ophthalmic procedures in some areas, and in several countries it is the most common elective surgery. In recent years, corneal refractive procedures have attracted increased public interest as the pursuit of uncorrected vision of 6/6 or better is on the rise. This may translate to an even greater demand for cataract and natural lens replacement in developed countries.
Natural lens replacement
Cataract surgery entails removing the cloudy natural crystalline lens of the eye. In natural lens replacement (NLR), the eye’s natural lens is not cloudy – the clear lens is removed and replaced with an IOL simply to change the focusing power of the eye. NLR can reduce or eliminate large amounts of ametropia and therefore may be a better surgical solution than laser vision correction for high prescriptions. In addition, presbyopia correction, using the latest technological advances in multifocal intraocular lenses, has proved to be something of a revolution for patients. It has allowed them to have their cataracts treated and then provided the opportunity to improve their distance, intermediate and near vision without glasses. The same intraocular lenses used for cataract surgery are used for NLR. Natural lens replacement is also known as RLE (refractive lens exchange) or CLE (clear lens extraction).
Modern day cataract surgery and NLR are identical procedures which require many manual steps and considerable skills of the ophthalmic surgeon.
Femtosecond laser
In recent years, femtosecond lasers have revolutionised the way in which we perform cataract/NLR surgery. Femtosecond laser-assisted cataract surgery provides surgeons with a new technological approach yielding even more predictable and refined results to what is already a remarkably safe and effective procedure. The femtosecond laser optimises the critical steps of cataract surgery, adding an element of precision that is unattainable with manual techniques.
A femtosecond laser has been successfully used for a number of years in Lasik (laser-assisted in situ keratomileusis). Here the laser technology is used as an alternative to manual and mechanical methods for creating reproducible and precise lamellar flaps.
The use of the femtosecond laser in cataract surgery and NLR allows the consolidation of the many skill-intensive steps of lens removal into a more predictable procedure resulting in improved outcomes.
From a surgical perspective, femtosecond lasers provide the following benefits:
- They create precise incisions in terms of size and architecture, which is important for the incision to seal appropriately without the use of stitches and to prevent infection. These incisions are stronger and have a better integrity than those created with a blade.
- They create a perfectly centred and sized capsulotomy through which the cloudy lens material is removed. The capsulotomy is more precise than those created manually and can take as little as 1.5 seconds to perform. As would be expected, an accurate capsulotomy with the femtosecond laser has been shown to result in better intraocular lens – anterior capsule overlap and hence better IOL positioning.
- They fragment the nucleus by liquefying, softening or ‘chopping’ the crystalline lens, in order to allow the lens material to be removed reducing the need for phacoemulsification.
- They create precise corneal incisions to correct pre-existing astigmatism which are more adjustable and quicker than manual techniques.
Femtosecond lasers work on the principle of photo disruption using a tightly focused beam of ultrashort pulsed light energy with enough peak power to create plasma. The plasma expands and causes a shock wave, cavitation, and bubble formation; the bubble expands and collapses, leading to separation of the tissue. Because femtosecond lasers function at a wavelength close to infrared, they are not absorbed by optically clear tissue. This makes femtosecond laser-assisted surgery amenable to anterior chamber targeting at various depths, as the anterior chamber provides an optically clear tissue space. The near-infrared wavelength is not absorbed by the cornea, and the waves are known to dissipate approximately 100μm from the lens tissue target.
There are currently five laser platforms available for commercial use for cataract/ NLR surgery:
- Catalys (Optimedica)
- LenSx (Alcon)
- Lensar (Lensar Inc)
- Victus (Technolas)
- Femto LDV-Z8 (Ziemer Ophthalmic Systems)
The main differences in these platforms are noted in table 1.
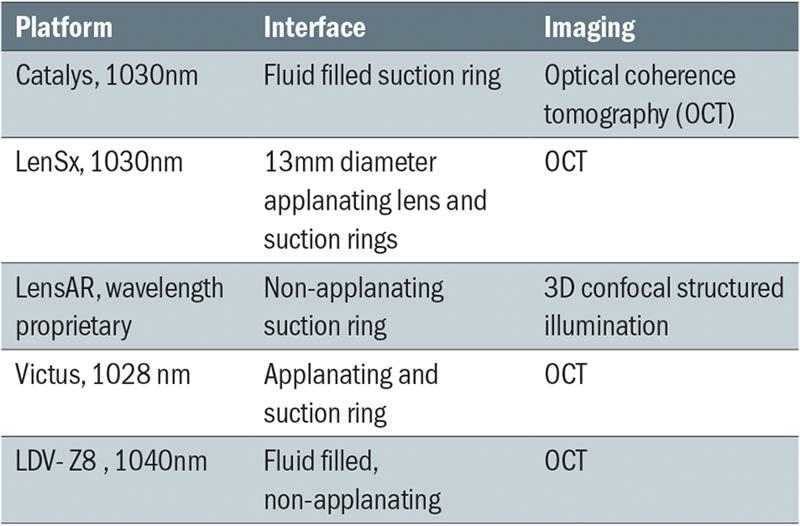
Table 1
Femtosecond procedure
Irrespective of which platform is used, the steps are essentially the same:
Docking (see figure 1)
For docking to occur, the patient must lie flat with the head positioned at a slight tilt to allow for the equipment to clear the nose. This step establishes the patient interface. There are two types of patient interfaces used by the laser platforms noted above, contact (applanating) or non-contact (fluid-filled interface), and each offers advantages and disadvantages.
Imaging
The anterior segment is imaged with either spectral-domain OCT or confocal structural illumination, a ray-tracing reconstruction of the anterior segment. The cornea must be centred within the applanated area to adequately centre the treatment. If the cornea is decentred, the primary clear corneal incision and arcuate incisions will not be appropriately positioned. This centration is important in all eyes but crucial in astigmatic patients in whom decentration could result in arcuate incisions within the visual axis or a wound posterior to the limbus. Those platforms using an OCT allows for real-time imaging of the ocular structures, eg the Catalys scans the entire cornea and the lens within the pupil to create a 3D image of the eye that is displayed in cross-section. There are sophisticated algorithms that process the OCT image, automatically and accurately detect the tissue surfaces. This creates safety zones to maintain adequate distance from the posterior capsule and iris and automatically compensates for any lens tilt or decentration from docking. The displayed images can be rapidly verified by the surgeon and customized if necessary.
Capsulorhexis
The capsulorhexis (sometimes spelled capsulorrhexis) is centred within the pupillary border and takes approximately 1.5 to 18 seconds to complete. The diameter of the capsulorhexis is approximately 5mm in most cases but can be modified according to pupillary dilation and IOL selection. Femtosecond laser capsulotomy has also been demonstrated to produce less IOL tilt and decentration as compared with manual continuous curvilinear capsulorhexis (CCC) yielding a more stable refractive result. The capsular opening is a critically important factor in determining effective lens position (ELP) which in turn, determines the effective power of the implanted lens (see figure 2).
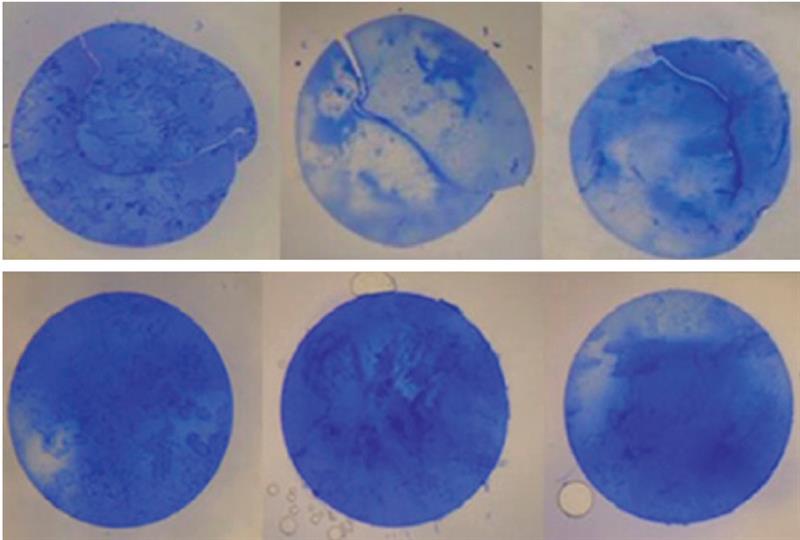
Figure 2: Manually opening the lens capsule (top) and opening the lens capsule using the Catalys laser (bottom)
Lens fragmentation
A grid pattern of lens fragmentation is optimised for each lens based on the density of the lens (selecting the number of segments; lens softening; cylindrical vs grid pattern) and to avoid accidentally applying photodisruption to the anterior or posterior capsule. Commonly used patterns include four, six or eight segments with or without the use of lens softening. Lens softening is performed in a cylinder pattern by some platforms and in a grid pattern by others. Lens tilt must be detected during imaging to help avoid accidentally involving these critical structures in the laser treatment. A default safety zone of 500 to 800μm is built in to the different platforms after imaging the anterior segment but may be adjusted. Laser time ranges from 30 to 60 seconds depending on the amount of lens softening selected (see figure 3).
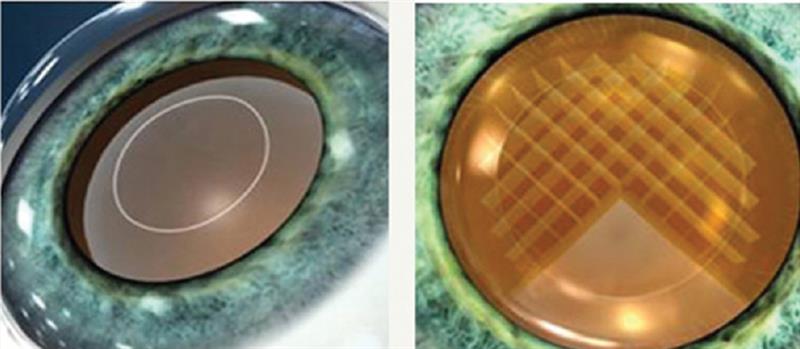
Figure 3: Catalys lens fragmentation
Corneal wound creation
Arcuate astigmatic correcting incisions (80% depth located at limbus by default but may be customised), paracentesis, relaxing incisions, and clear corneal wounds can be created by the femtosecond laser platforms. The wounds have been shown to be stable and watertight with minimal anterior chamber reaction for up to a few hours.
The total duration of laser treatment lasts from 30 seconds to three minutes depending on the steps performed, the lens density and grid pattern, and softening option that is chosen.
Once the laser treatment has been completed, the suction is released, the patient interface is removed, and the patient is slowly undocked from the laser. Depending on whether the laser is located in the operating room or in another location, the surgeon can proceed with phacoemulsification.
Clinical results
The following are the clinical results from a study done at Optical Express to evaluate the Catalys femtosecond laser versus manual natural lens replacement. The study included a stratified random sample of an equal number of Catalys and manual patients (n=200). Results were collated one month post-procedure. All procedures were performed by a senior surgeon, David Teenan, at the Optical Express IOL treatment clinic in Glasgow. Dr Teenan has done in excess of 10,000 IOL procedures. All patients had the Tecnis Symfony multifocal IOL implanted.
For the Catalys procedures, the capsulotomy diameter was 5.0 ±0.32mm (4.3 to 8.0) and the lens fragmentation pattern was a grid and quadrant pattern. The dataset is noted in table 2.
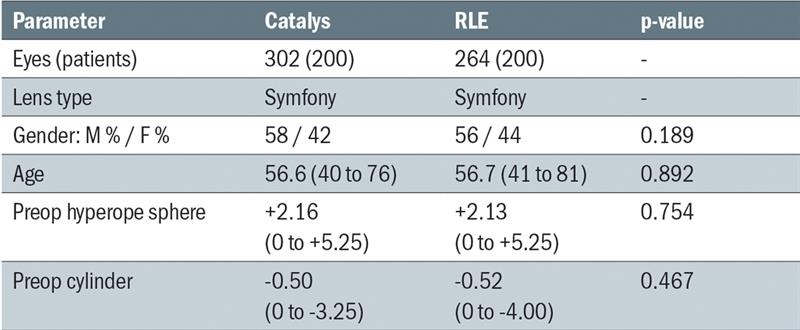
Table 2
Figures 4 to 7 demonstrate that the Catalys femtosecond procedure produced better uncorrected distance visual acuity despite very similar refractive predictability. Patient satisfaction, recommendation of the procedure and uncorrected near visual acuity were similar in the Catalys femtosecond procedure and the manual procedure.
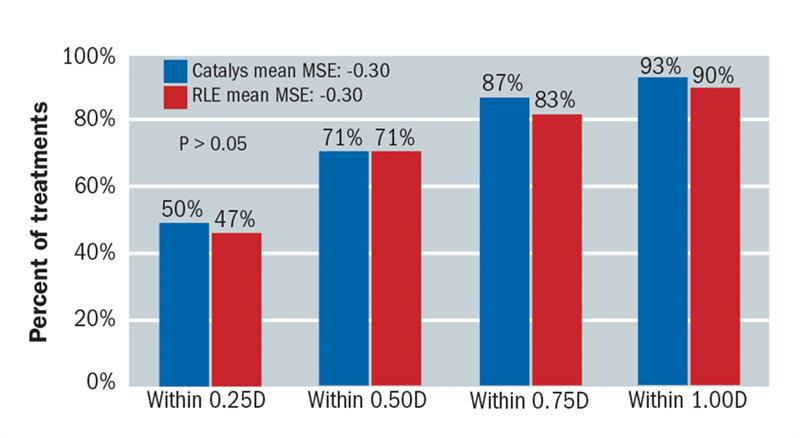
Figure 4: Month 1 within target (MSE predictability)
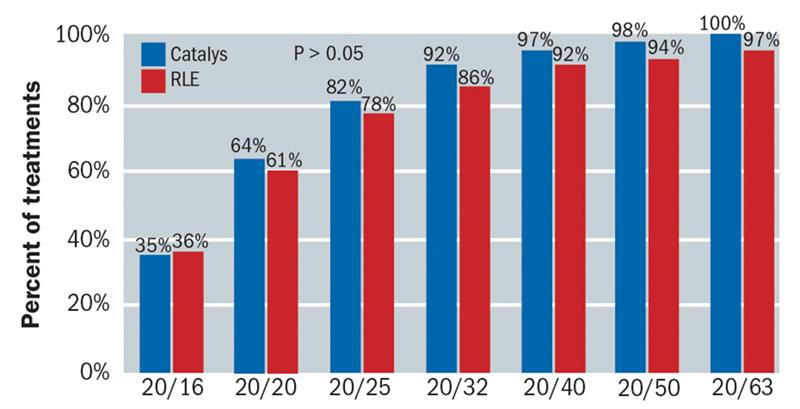 Figure 5: Month 1 uncorrected distance visual acuity distribution
Figure 5: Month 1 uncorrected distance visual acuity distribution
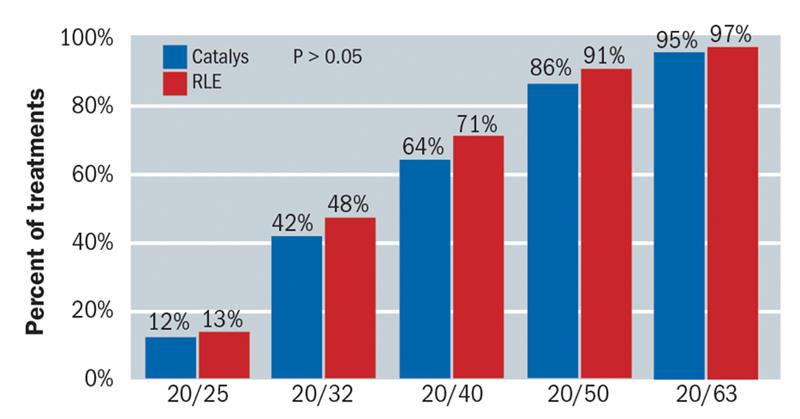 Figure 6: Month 1 uncorrected near visual acuity distribution
Figure 6: Month 1 uncorrected near visual acuity distribution
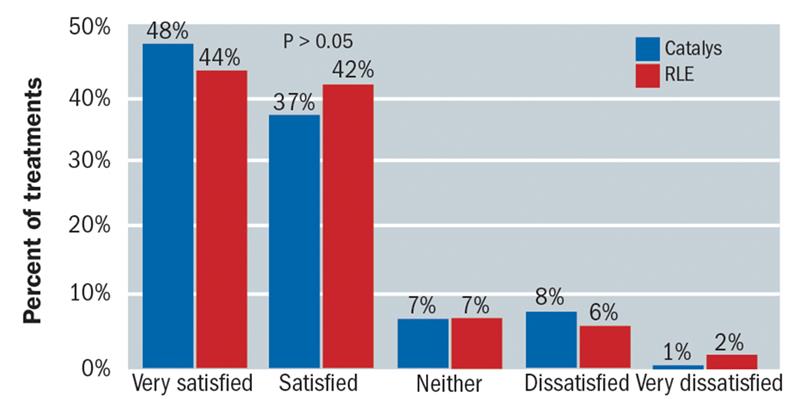 Figure 7: Patient satisfaction rating
Figure 7: Patient satisfaction rating
This was a well matched study which treated patients in the same centre and by the same surgeon. The sample size was reasonable (302 eyes with the Catalys and 264 eyes with the standard procedure) and the outcomes demonstrated improved unaided vision with the Catalys. As a testament to the already impressive outcomes of the standard procedure, larger studies would be needed, and in fact are under way, to show improvements in other aspects of the procedure, such as the refractive outcome and the potential for complications.
Conclusion
Although femtosecond procedures have become the standard of care at Optical Express, the current price point prohibits its use on the NHS and by many private providers of cataract and NLR procedures. However, with the development of premium intra-ocular lenses like the Tecnis Symfony IOL, patients are increasingly willing to invest in technology that could potentially fulfil the increased expectation of achieving 6/6 vision or better, coupled with safety, efficiency and reproducibility.
Femtosecond laser-assisted cataract/NLR surgery seems to be a safe, efficient, and reproducible procedure, but more prospective randomised studies will further demonstrate the potential clinical benefits of this emerging technology.
Dasi Raju is clinical director at Optical Express.