We recently published two papers from the team at Aston University looking at the influence of nutrition and nutritional supplements upon the progression of age related macular degeneration.
The first article - click here to read it - included the following important points;
- Nutrients that have been investigated as possibly influencing the course of AMD include zinc, omega-3 fatty acids, vitamin C, vitamin E and the carotenoids which have vitamin A activity and include the diet-originated macular pigment xanthophylls lutein and zeaxanthin (along with meso-zeaxanthin converted at retinal level)
- The AREDS formulation of vitamin C 500mg, vitamin E 400IU, b-carotene 15mg, and zinc (zinc oxide 80mg and cupric oxide 2mg) showed a 25% risk reduction in progression to advanced AMD over five years in patients with intermediate AMD (extensive intermediate drusen in one or both eyes, one or more large drusen in at least one eye, or non-subfoveal geographic atrophy in one eye) or advanced AMD (subfoveal geographic atrophy or choroidal neovascular membrane) in one eye.
- The AREDS formulation showed no effect in preventing the development of large drusen in participants who had small drusen at baseline.
- Because of the high dosage of zinc, and the inclusion of beta-carotene (linked with lung cancer in smokers), some eye professionals became concerned with the safety of the formulation and were reluctant to advise patients to use it.
- AREDS2 found that adding lutein and zeaxanthin to the original formula did not further reduce the risk of progression to advanced AMD. However, a subset of participants who took the AREDS formulation with beta-carotene substituted out for lutein and zeaxanthin, had their risk of progression to advanced AMD reduced by 18% compared to those participants who took the AREDS formulation that contained beta-carotene but no lutein and zeaxanthin. In addition, participants who had ≤ 0.823 mg per day dietary intake of lutein and zeaxanthin at the start of the study, but who took the AREDS 2 formulation, were 25% less likely to develop advanced AMD compared with participants with similar dietary intake who did not take the supplementation
The second article - click here to read it - included the following points;
- lutein and zeaxanthin are the most beneficial nutrients for AMD
- lutein and zeaxanthin can only be obtained in the diet (are not synthesised by the body)
- the most lutein and zeaxanthin rich foods are spinach, kale and eggs
- the AREDS2 formula is the only clinically proven supplement
- the AREDS2 formula has only been found to be beneficial when the disease is at a certain stage
It is important for you to be familiar with these reference sources before your discussion. You may also wish to familiarise yourself with the AREDS2 paper by clicking here.
Once you have read through the source material, please attempt the six multiple choice questions on the following page.
..................
MCQS
........................................
Now consider the following case.
Case study
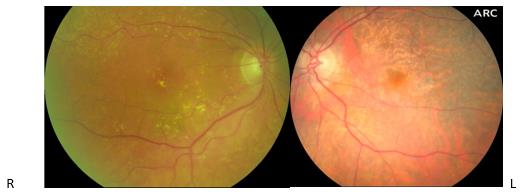
A 76 year old female patient is seeing you for an annual eye examination. She has already been diagnosed with dry age related macular degeneration in both eyes and has been discharged from hospital with the advice to have annual eye examinations in community practice.
Best corrected acuity; R 6/7.5 L 6/36
Her right eye shows extensive intermediate drusen and early nucleosclerotic cataract and in her left pseudophakic eye there is extensive subfoveal geographic atrophy.
She is happy with her overall level of vision. She has no significant general health concerns and is not taking any current prescription medicines.
She has read that ‘there may be some vitamin tablets that might help improve her vision.’
To gain your CET point you are required to discuss the following with another GOC registered practitioner and consider the following;
What advice regarding nutrition might you give to this patient? Please make sure that your advice is supported by the published evidence.
Remember, there may be a divergence of views – we simply need to know what you and your colleague think and why.
Remember, your interaction should last for at least 10 minutes (and completion of the submission will be taken as your statement that this is true) and you will be required to submit the outcome of your discussion along with the name and GOC number of the person with whom you have interacted with.
Once you submit your responses, our review team will either;
- Confirm completion and an interactive CET point
- Ask by email for further clarification
- Suggest that too little information was submitted this time for a point to be awarded.
- At the end of the month’s active period we will confirm that your discussion outcome meets the requirement for an interactive point
NAME AND GOC NUMBER OF CORRESPONDENT
And the outcome of your discussion
WHAT ADVICE IS APPROPRIATE?