
Retinal Contusion and Angle Recession
During the lockdown, we were all encouraged to exercise and keep fit in general. Lots of us tried walking, running and cycling to keep fit. Others tried resistance exercises, to build up muscle and tone arms and legs. Here I describe an incident of blunt trauma to an eye due to resistance band recoil.
Case 1
At the start of the lockdown, 25-year-old male, MB, was undertaking routine strength exercises using a resistance band. Ingeniously, he tried to use a wooden cricket stump to perform the arm resistance work out. Unfortunately, the wooden stump snapped and the resistance band recoiled at great speed and with force upon his left eye. He ‘blanked out’ for a few seconds and could not remember the actual moment of impact, but came round to a very painful, swollen left eye through which he was unable to focus. The patient’s mum rang our practice late in the evening to report the incident. My advice was to go straight to Western Eye hospital and he was seen there as an emergency admission.
Initial management; hospital
MB was prescribed the following:
- Dorzolamide/timolol (Cosopt); drops, 2x a day
- Dexamethasone (Maxidex); drops, hourly
- Chloramphenicol; 4x a day
- Cyclopentolate 1.0% (Mydrilate); 3x a day
MB had been under my care since age five, over which time enough of a rapport had grown for both mother and son, on this occasion, to seek my advice about his hospital management and whether they should seek a private ophthalmology consultation. Due to the traumatic origin of his injury, I advised MB to try to lie flat and avoid vigorous movement before seeing me.
Clinical findings; three days post-trauma
- Visual acuity;
- R; 6/6 (N5)
- L; count fingers at 30cm using peripheral vision
- Right eye anterior and posterior examination revealed no abnormalities.
- Anterior assessment (figure 1);
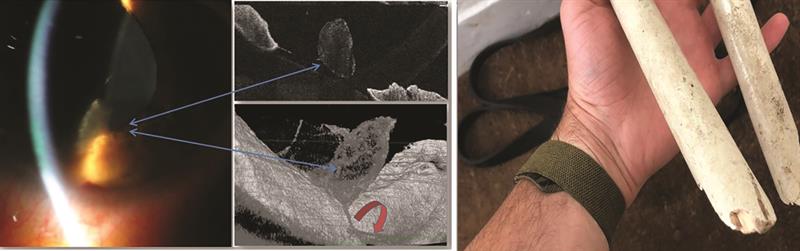 Figure 1: Slit-lamp and anterior OCT images of left eye at three days post-trauma. Slit-lamp image (left) shows a ball of fibrous tissue and hyphaema in the inferior angle. Anterior OCT shows the fibrous ball floating just above the crystalline lens (blue arrows, centre images) and hyphaema (red arrow, centre bottom image). Note the inflammatory fibrils seen as white lines and spots within the pupil. The broken wicket stump that caused the recoil is seen on the right
Figure 1: Slit-lamp and anterior OCT images of left eye at three days post-trauma. Slit-lamp image (left) shows a ball of fibrous tissue and hyphaema in the inferior angle. Anterior OCT shows the fibrous ball floating just above the crystalline lens (blue arrows, centre images) and hyphaema (red arrow, centre bottom image). Note the inflammatory fibrils seen as white lines and spots within the pupil. The broken wicket stump that caused the recoil is seen on the right
- Right; no abnormalities
- Left;
- Corneal swelling; corneal thickness at 675μ (compared to 558μ in the right eye)
- A ball of fibrous material seen floating in anterior chamber
- Iris hyphaema
- Intraocular pressures in left eye; 20mmHg (reduced from 33mmHg since using Cosopt)
- Posterior chamber (figure 2);
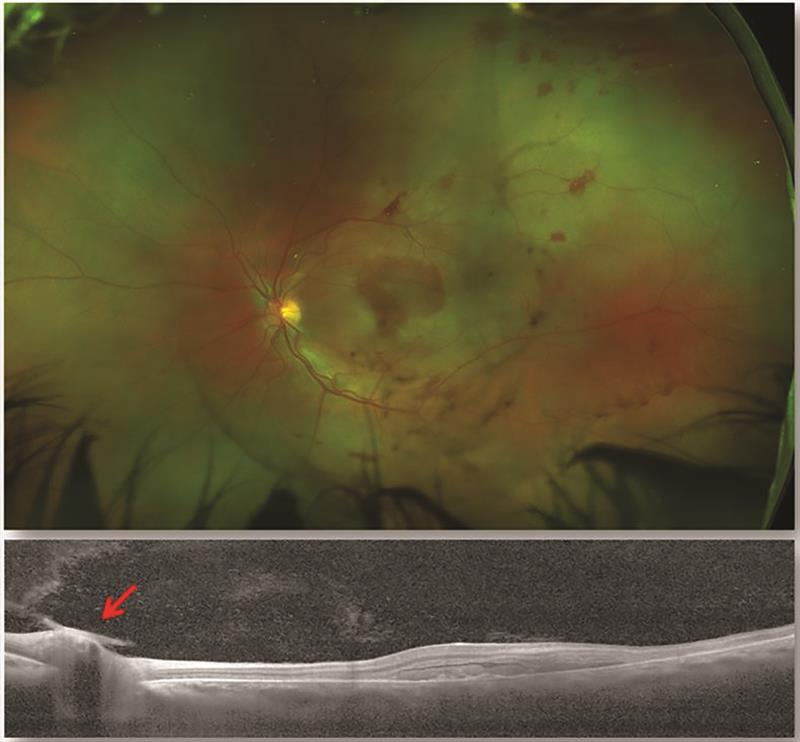 Figure 2: Optomap wide field image (top) and OCT retinal scan (bottom). Fundus shows signs of traumatic retinopathy. Retinal concussion has caused the appearance of white patches due to oedema, seen in the central, superior temporal and nasal paracentral areas. A cherry red spot is seen at the fovea. Vitreous haemorrhages are seen as black lines, and the presence of large blot intraretinal haemorrhages implies contusion as well as concussion. The OCT scan retinal swelling due to haemorrhage and disruption of the photoreceptor and retinal pigment epithelial layers. The red arrow indicates vitreous haemorrhage just above the disc. Central macular thickness was measured to be 482µ, suggesting oedema
Figure 2: Optomap wide field image (top) and OCT retinal scan (bottom). Fundus shows signs of traumatic retinopathy. Retinal concussion has caused the appearance of white patches due to oedema, seen in the central, superior temporal and nasal paracentral areas. A cherry red spot is seen at the fovea. Vitreous haemorrhages are seen as black lines, and the presence of large blot intraretinal haemorrhages implies contusion as well as concussion. The OCT scan retinal swelling due to haemorrhage and disruption of the photoreceptor and retinal pigment epithelial layers. The red arrow indicates vitreous haemorrhage just above the disc. Central macular thickness was measured to be 482µ, suggesting oedema
- Right; no abnormalities
- Left;
- Vitreous haemorrhaging
- Suspicion of cells in posterior chamber
- Optomap fundus examination showed haemorrhaging indicative of commotio retinae
- Cherry red spot (seen centrally against the white background) indicating retinal contusion
- Centrally there appeared to be a large intraretinal haemorrhage and both multiple intra- and pre-retinal haemorrhages around the posterior pole
Clinical Findings – 10 days post-trauma
Left eye findings:
- Visual acuity; 2/150.7 (peripheral viewing)
- Pupils; left pupil dilated (traumatic mydriasis seen as anisocoria) and unreactive to direct, consensual or near reflex
- Left anterior chamber (figure 3);
- Central corneal thickness; 564µ (a reduction of 111µ from last measurement)
- Complete resolution of hyphaema
- Angle recession visible
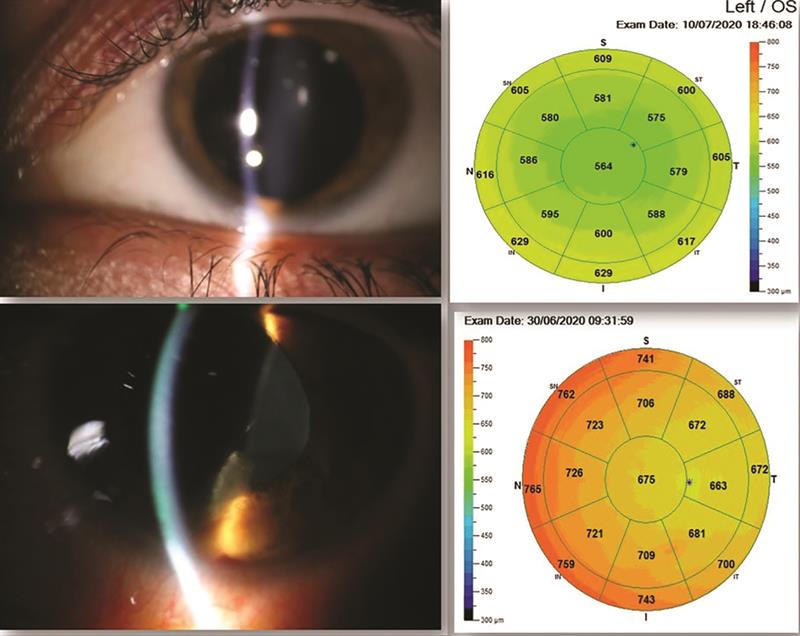 Figure 3: Anterior left eye at 10 days post-trauma (top images) showing full resolution of hyphaema, no inflammatory activity and reduction in corneal thickness from previous measurements (bottom)
Figure 3: Anterior left eye at 10 days post-trauma (top images) showing full resolution of hyphaema, no inflammatory activity and reduction in corneal thickness from previous measurements (bottom)
- Posterior chamber (figure 4);
- Optomap ultrawide field imaging showed resolution of the vitreous and posterior pole intraretinal haemorrhages. A deep red bleed, superior to the fovea, can be seen indicating haemosiderosis changes to the blood
- Optomap autofluorescence imaging revealed central hypofluorescence and a ring of hyperfluorescence, both indicating increasing metabolic activity following the trauma
- OCT scan revealed shearing of the inner retina with disruption to the layers of both the inner and outer retina.
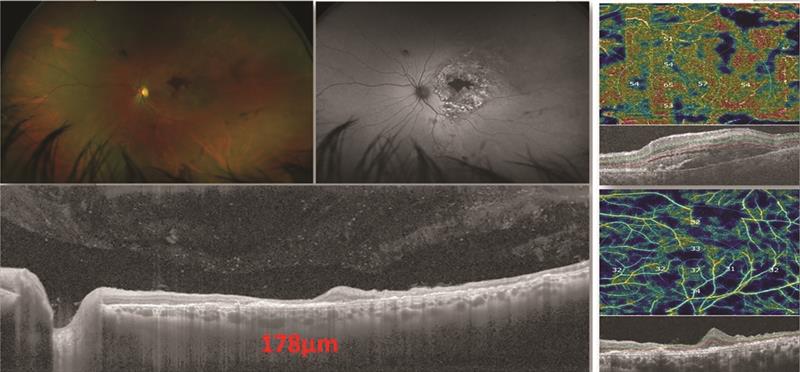 Figure 4: Retinal appearance ten days post-trauma. The vitreous and intraretinal blot haemorrhages have resolved, but the colour image (top left) shows darkening of the blood centrally indicating possible haemosiderosis. Autofluorescence image (top central) indicates lipofuscin activity indicated by the bright hyperfluorescent spots. The OCT image (bottom left) shows residual vitreous vascular debris, while the optic disc appears to show normal cupping. Macular thickness now measures 178µ (a drop from 304µ), while the RPE and photoreceptor layers show some disruption. The elevated region is due to intraretinal haemorrhaging. OCT-angiography (right column images) reveal the earlier surface haemorrhaging and swelling (top right) and resolution (bottom right)
Figure 4: Retinal appearance ten days post-trauma. The vitreous and intraretinal blot haemorrhages have resolved, but the colour image (top left) shows darkening of the blood centrally indicating possible haemosiderosis. Autofluorescence image (top central) indicates lipofuscin activity indicated by the bright hyperfluorescent spots. The OCT image (bottom left) shows residual vitreous vascular debris, while the optic disc appears to show normal cupping. Macular thickness now measures 178µ (a drop from 304µ), while the RPE and photoreceptor layers show some disruption. The elevated region is due to intraretinal haemorrhaging. OCT-angiography (right column images) reveal the earlier surface haemorrhaging and swelling (top right) and resolution (bottom right)
Visual field (figure 5); central loss with some residual around 15 degrees temporally and also superioronasally
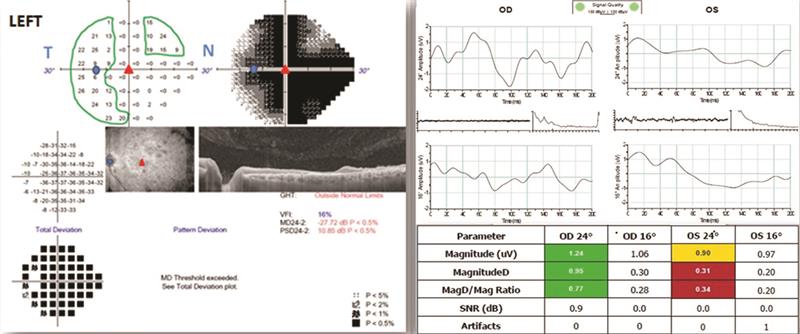 Figure 5: Left visual field plot (left) showing central loss and a nasal step due to ganglion cell and nerve fibre damage. Areas of residual vision are outlined in green. Pattern ERG concentric stimulus fields (right) show response to high contrast 24 and 16 degree stimuli. This is outside normal parameters and is due to ganglion cell damage in the foveal, parafoveal and paracentral regions
Figure 5: Left visual field plot (left) showing central loss and a nasal step due to ganglion cell and nerve fibre damage. Areas of residual vision are outlined in green. Pattern ERG concentric stimulus fields (right) show response to high contrast 24 and 16 degree stimuli. This is outside normal parameters and is due to ganglion cell damage in the foveal, parafoveal and paracentral regions
- Electroretinography (ERG, figures 5 and 6);
- Concentric field stimulus revealed damage to the central ganglion cells and a reduced Mag D to Mag ratio.
- Note of interest; the right eye ERG was normal, although the waveform was not the typical 3 peak steady wave form. This would indicate that there was some shaking effect or sympathetic reaction from the right eye following the blunt trauma
- ERG flicker test (figure 6); appeared normal, indicating that even though there was metabolic activity happening on the retina as seen with autofluorescence, there was no indication of early ischaemic retinopathy.
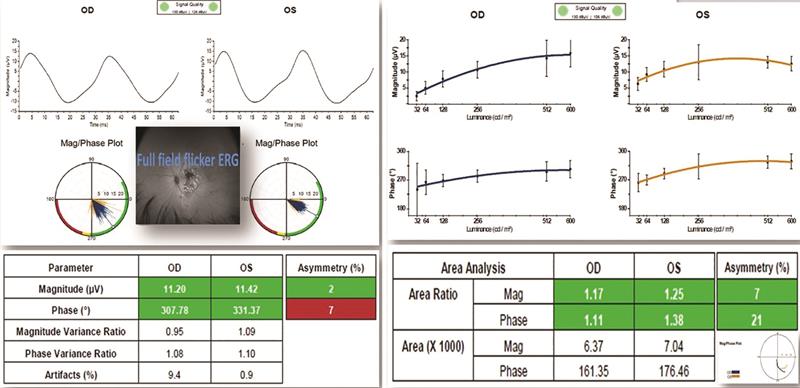 Figure 6: Full field flicker ERG response to fixed luminance and multi-luminance stimuli. This is a measure of cone function across the full field rather than just the macular area and is useful for obtaining objective data from ischaemic retinal disorders, such as diabetic retinopathy and central retinal vein occlusion. These results show that both eyes have good amplitude and phase response. The greater the number of cones that respond to stimuli, the higher the energy and greater the amplitude of response. The phase is a measure of consistent timed responses with each light stimulus and, here, shows good phase, confirming there to be no propensity for ischaemic retinopathy
Figure 6: Full field flicker ERG response to fixed luminance and multi-luminance stimuli. This is a measure of cone function across the full field rather than just the macular area and is useful for obtaining objective data from ischaemic retinal disorders, such as diabetic retinopathy and central retinal vein occlusion. These results show that both eyes have good amplitude and phase response. The greater the number of cones that respond to stimuli, the higher the energy and greater the amplitude of response. The phase is a measure of consistent timed responses with each light stimulus and, here, shows good phase, confirming there to be no propensity for ischaemic retinopathy
Discussion
There are 2.5 million ocular injuries annually, and males tend to be nine times more likely to suffer injury than females. Most ocular injuries are seen in patients below the age of 40.
Commotio retinae
Commotio retinae, a Latin term that translates as ‘disturbance or the retina,’ was first described by the German ophthalmologist Rudolf Berlin and the condition is still sometimes described as Berlin’s oedema. Commotio retinae describes a retinopathy secondary to direct or indirect trauma to the globe. It is a concussive disorder caused by pressure shock waves transmitted through the eye subsequent to external blunt trauma. The energy of the compressive wave then damage to the outer retina and particularly the photoreceptors.
Ophthalmoscopy reveals a sheen-like retinal whitening some hours after the initial injury. Retinal opacification is thought to be due to extracellular oedema, glial swelling and photoreceptor outer segment disruption. Some theories suggest that it is due to pigment epithelium disruption, but auto-fluorescence shows no hyperfluorescence as would be the case with RPE active changes. In this patient’s case, the severity of the damage to the RPE did show as hyperfluorescence a fortnight later.
Commotio retinae can be divided into two categories:
- Retinal concussion; a milder form. Vision is usually 6/60 or better and prognosis of good visual recovery within two to four weeks is expected. Grey/white retinal opacification is less dramatic, and there is no obvious retinal vessel leakage.
- Retinal contusion; more severe damage. Vision loss can be mild to severe, and if macula is affected, the loss of acuity is usually permanent. The retinal whitening is more intense and usually associated with retinal and/or vitreous haemorrhages. Severe cases are also associated with pigmentary changes and retinal atrophy.
Anterior-posterior compression of the globe at the cornea reduces axial length by up to 40%, while the equatorial diameter increases by as much as 125%. This equatorial elongation causes shearing forces between the expandable outer wall and the much less distensible vitreous.
Angle recession
Angle recession is a common manifestation of blunt trauma injury to the eye and is due to a rupture of the ciliary face resulting in a tear between the longitudinal and circular fibres of the ciliary body (figure 7). The longitudinal fibres are still attached to the scleral spur, and there is a retrospective displacement of the iris root and circular muscles. The anterior chamber becomes deep due to posterior deviation of the relaxed iris-lens diaphragm.
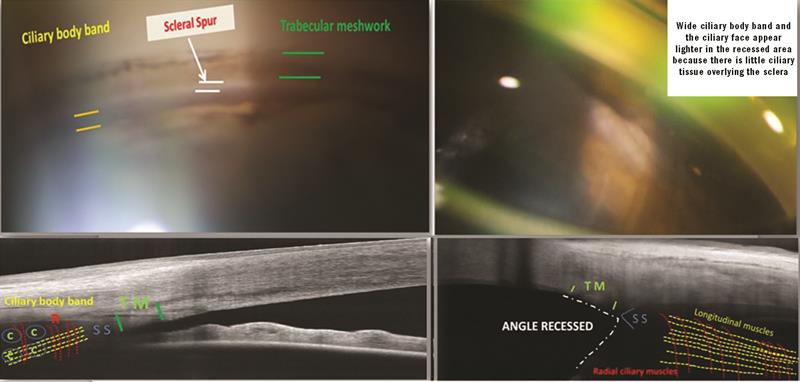 Figure 7: Gonioscopy image (top left) of the normal angle showing the pigmented anterior and posterior trabecular meshwork, scleral spur, ciliary body band and iris. Anterior OCT (bottom left) shows a normal trabecular meshwork (TM), scleral spur (SS), iris and ciliary body band. Schematic overlay of longitudinal (yellow dashed lines), radial (red R) and circular (C in blue circle) muscle fibres is added to the left of the image. The top right image shows a recessed angle following a blunt trauma. This is seen using anterior OCT (bottom right) where the recessed angle is shown together with the tear in the circular muscle fibres. These are displaced posteriorly while the longitudinal fibres remain attached to the scleral spur resulting in the iris root being dragged downwards
Figure 7: Gonioscopy image (top left) of the normal angle showing the pigmented anterior and posterior trabecular meshwork, scleral spur, ciliary body band and iris. Anterior OCT (bottom left) shows a normal trabecular meshwork (TM), scleral spur (SS), iris and ciliary body band. Schematic overlay of longitudinal (yellow dashed lines), radial (red R) and circular (C in blue circle) muscle fibres is added to the left of the image. The top right image shows a recessed angle following a blunt trauma. This is seen using anterior OCT (bottom right) where the recessed angle is shown together with the tear in the circular muscle fibres. These are displaced posteriorly while the longitudinal fibres remain attached to the scleral spur resulting in the iris root being dragged downwards
Angle recession is often masked initially by hyphaema that results from anterior ciliary artery shearing damage. Angle recession is found after a traumatic hyphaema in 85% of cases, and 11% of eyes with identifiable angle recession will go on to develop a secondary glaucoma. Interestingly, 50% of eyes with angle recession glaucoma and optic neuropathy may develop sympathetic glaucoma in the uninjured eye.
Blunt force to the globe causes equatorial distension with anterior to posterior axial compression. Sudden indentation of the cornea forces aqueous to be displaced posteriorly and laterally, deepening the anterior chamber and increasing the diameter of the corneal scleral limbal ring. The shearing forces to the drainage angle result in a tear between the longitudinal and circular fibres of the ciliary muscle. The longitudinal muscle insertion at the scleral spur remains intact, while the circular muscle is displaced posteriorly along with the iris root and pars plicata.
The shock waves causing angle recession can also result in pupillary sphincter tears, iridodialysis, cyclodialysis and zonular tears.
Intraocular pressures may rise immediately after the injury as a result of hyphaema (blood accumulating in the anterior angle restricts aqueous outflow) or from other comorbidities, such as iridocyclitis or pupillary block from ectopia lentis. Red blood cells, pigment cells and inflammatory cells may also obstruct the trabecular meshwork and raise pressures.
Secondary glaucoma can also result from subsequent degenerative changes and scarring of the traumatised trabecular meshwork leading to obstruction of the aqueous outflow.
Gonioscopy should be deferred for six week after acute injury and this should now reveal any asymmetry of the angle recess or widening of the ciliary body band due to retro displacement of the iris root.
Traumatic mydriasis and anisocoria
Blunt trauma to the eye or globe can result in a traumatic mydriasis, whereby the affected pupil is dilated and loses direct, consensual light or near convergence pupil reflexes (figure 8). David Bowie was a famous sufferer of such. Usually permanent, traumatic mydriasis occurs due to tears in the sphincter muscle fibres of the iris. Contusion can also lead to temporary mydriasis, while direct blunt trauma to the iris sphincter muscles can lead to permanent traumatic mydriasis.
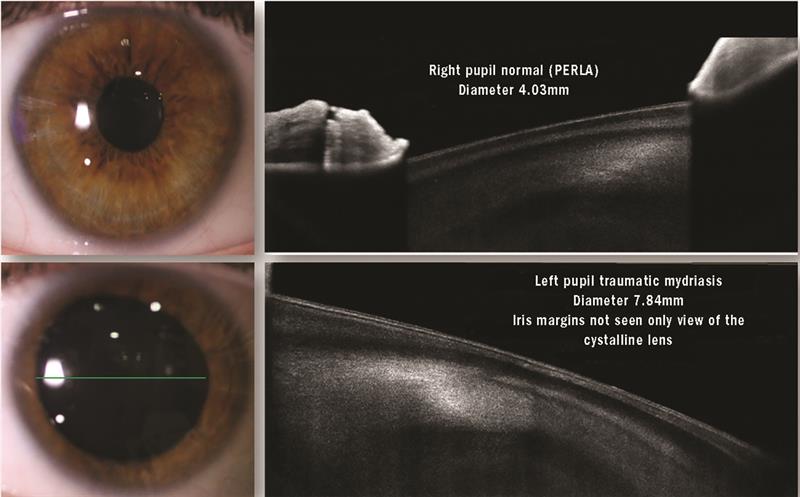 Figure 8: Traumatic mydriasis (lower images) causing anisocoria (compare top and bottom images) following blunt trauma
Figure 8: Traumatic mydriasis (lower images) causing anisocoria (compare top and bottom images) following blunt trauma
Kirit Patel is an optometrist in independent practice in Radlett, Hertfordshire.

