On the very morning that I was due to try out the new Heidelberg Spectralis Spirit for the first time, the latest guidelines from NICE were announced concerning the diagnosis and management of age-related macular degeneration.
Though it might be argued there was little of surprise in the new guidelines, one sentence stood out to me: ‘If you suspect late AMD (wet active), you may offer OCT to decide whether to refer for further investigations, including FFA, provided that you have been trained to interpret the data and feel competent to do so.’ If indeed it were needed, this is good evidence that the OCT is now an accepted part of community eye care instrumentation and, as the largest multiple chain introduce OCTs, it cannot be long before the majority of practices offer OCT.
Community practice
When first confronted with a modern OCT, such as Heidelberg Spectralis for example, the range of scans and analyses can be quite daunting. The laser can centre upon the macula, the disc or the cornea and scan in a number of ways, such as:
- as a single line – capable of showing a high resolution cross section of tissue (figure 1)
- radial (star-shaped) scan – able to measure, for example, corneal or retinal thickness (figure 2)
- volume scan – a multiple line scan through a block of tissue allowing a 3D representation of retina which can be looked through slice by slice to highlight individual structure changes (figure 3)
- annular scan – a circle scan around a structure such as the disc able to show thickness of tissues around the disc and so able to define areas of retinal nerve fibre layer (RNFL) thinning as might occur in glaucoma (figure 4)
The incident confocal light is able to generate a scanning laser ophthalmoscopy image of the retina (figure 5), which some systems offer in colour, or as en face representations of different layers.
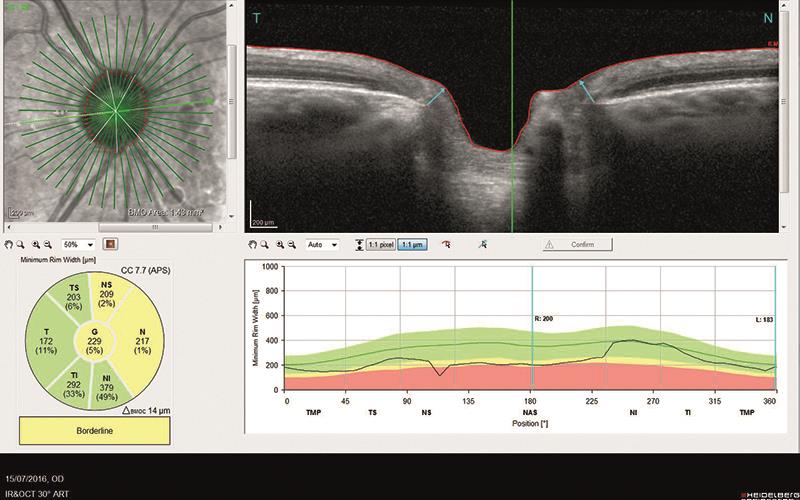
Figure 2
Data gathered can be represented in a multiplicity of ways, such as the colour thickness map (figure 2) or RNFL ‘twin peaks’ map (figure 4), and serial assessment of the patient may be analysed to detect any differences in structure over time which may be displayed as difference maps.
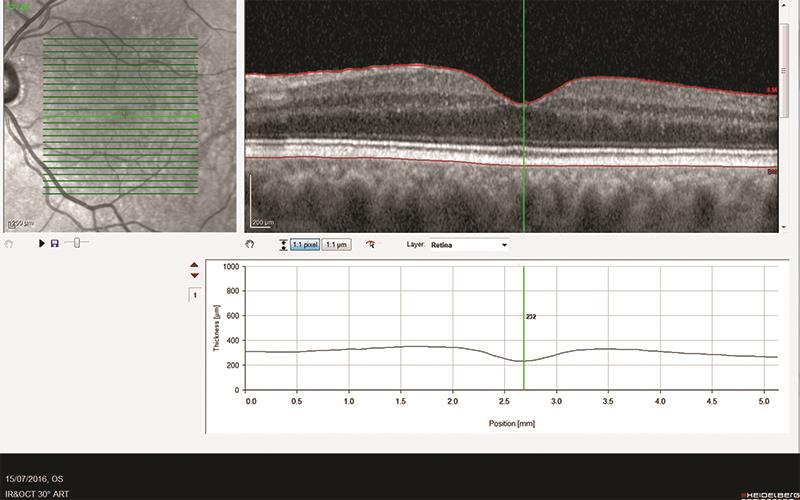
Figure 3
Many OCTs have been incorporated into practices already involved in enhanced care services and where particular programming and data outputs are already specified.
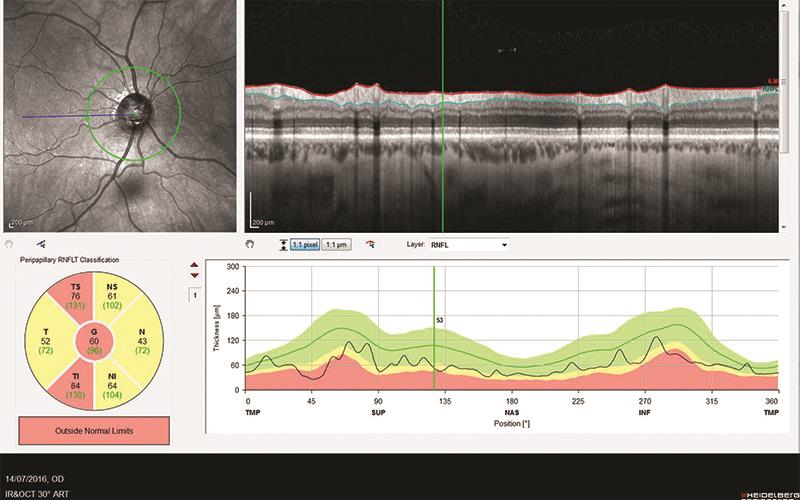
Figure 4
With experience, the trained user is also able to select the appropriate capture and display for individual patient presentations. That said, the increased interest in OCTs for general community practice has meant that there is a place for an OCT that can offer the essential data capture options but could easily be upgraded at a future date if further capability was required.
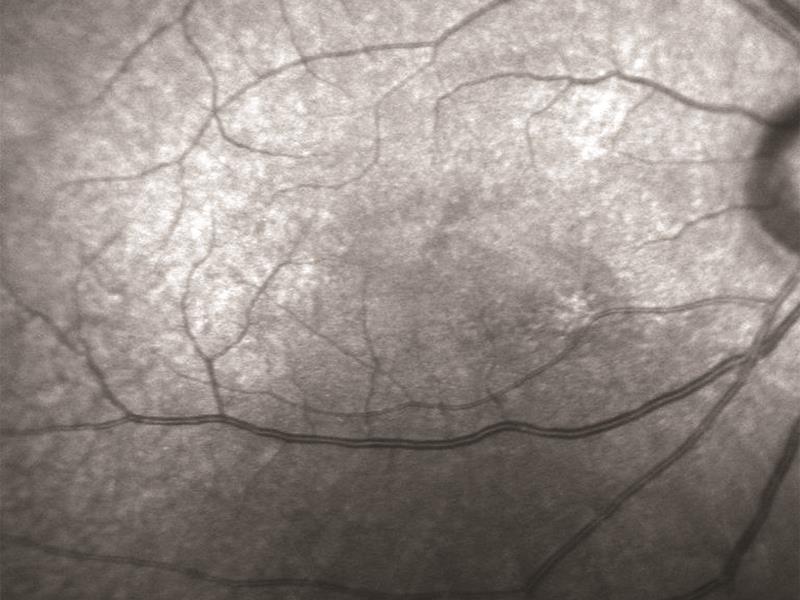
Figure 5
Heidelberg Spirit
The new Heidelberg Spectralis Spirit has been designed for the optometrist working in community practice.
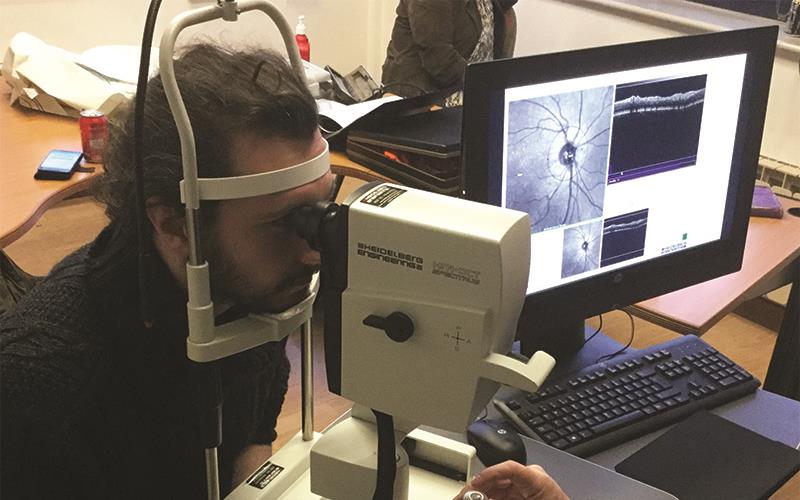
Figure 6
The unit looks similar to the Spectralis (figure 6), and indeed can be upgraded at any time to offer the full range of Spectralis functions, but has been adapted to offer those functions most likely to be required in community practice eye examinations. These include:
- a volume scan off the retina centred at the macula – essential for detecting retinal thinning (as might occur with atrophic diseases or glaucoma)
- an annular scan around the disc – essential in glaucoma screening
- a comparison of current data with existing data to highlight any change in structure over time
- an anterior scan option (with the application of a supplementary lens) is now available, along with a pseudo colour option that makes the cSLO scan look familiar to patients
Ease of use
I was impressed by a number of new features making operation easy. Indeed, a retinal and disc analysis of both eyes, even on some trickier patients, was quite possible within just four minutes. This is worth noting if anyone is thinking of offering OCT as part of a screening option within a routine eye assessment.
Firstly, setting up is simple with the patient data input simplified and requiring just the selection of one or both of the two operations. I used the default setting offering first retinal and then disc scanning. You then start the capture process and move the unit towards the pupil until the retina is visible on screen.
The patient views a blue light (low intensity and, unlike many instruments I have tried, not bright enough to cause any patient discomfort) which is first macula-centred, then moves to detect the disc so allowing reference points for the volume scan to be undertaken. Focusing is helped by an option to put in the refractive error of the patient and there is also a ‘long eye’ option for high myopes.
Particularly helpful was an onscreen indicator if too close or too far away from the patient (figure 7). Once in focus, the cross section is seen in a separate window and the image quality is indicated with a sliding scale.
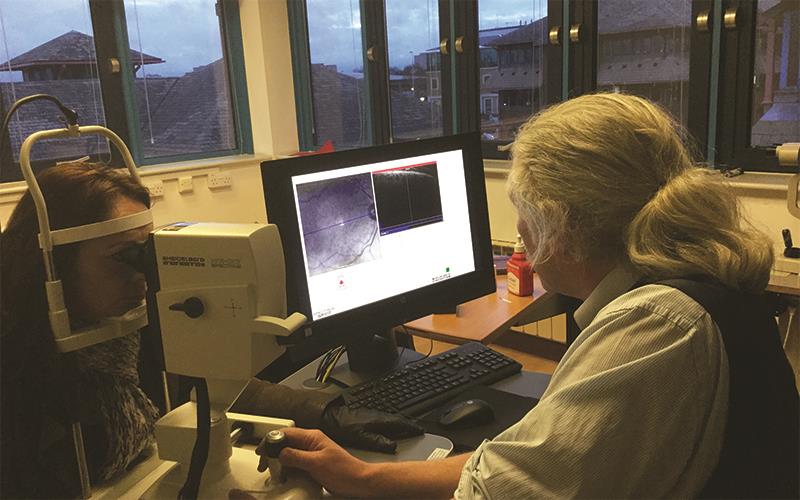
Figure 7
Capture (by pressing the joystick button) then follows and the accurate Heidelberg tracking means that capture is stopped whenever the patient moves their eye. In all, 61 raster scans are undertaken and these are counted up onscreen so it is easy to see how you are progressing. Then onto the disc which, after centring, is completed within seconds.

Figure 8
The new software includes the Heyex system which makes all the data compatible with tablet displays. This is important as it means that the data may be displayed and analysed in any consulting room with a tablet networked to the main OCT unit (figure 8). Figure 9 shows a tablet display for one of my patients where an area of retinal thinning had been identified.

Figure 9
Clinical relevance
Thankfully, there is wider acceptance in the ophthalmology community now for optometrists having access to OCTs and, indeed, the NICE guidelines support this. Initial reticence was based upon a fear of over-referral from optometrists of suspect cases which were, in fact, either poor quality scans or ones where the traffic light system had flagged up an anomalous structure of, for example, congenital origin as a possible disease process.
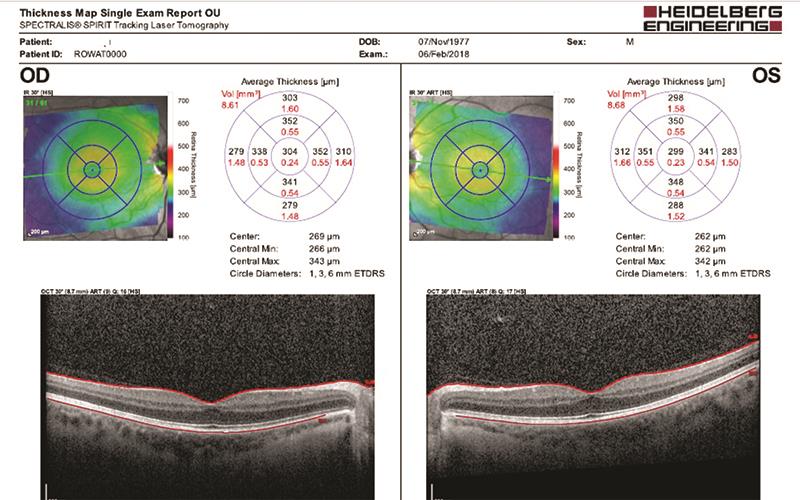
Figure 10
The Spectralis Spirit addresses this concern a number of ways. Most obvious of these is the ease of capture which makes accurate scans very easy for all to obtain. Secondly, the data captured is displayed in a few simple options. Figure 10 shows the results for each eye of one patient in my trial. Thickness values across the central retina are clearly displayed along with a colour coded thickness map (blue for thin, red for thick) and a cross section image of the retina. Figure 11 shows the RNFL data for the same patient.
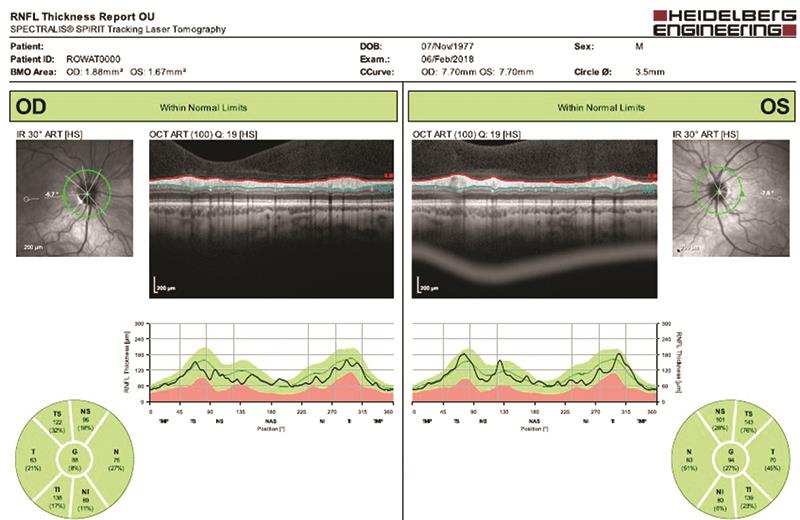
Figure 11
The twin peak plot is still present as is colour coding (green suggests normal values here – anything outside the expected normative database values, as in figure 12, are shown as red and there is no amber option, again to simplify things for the clinician).
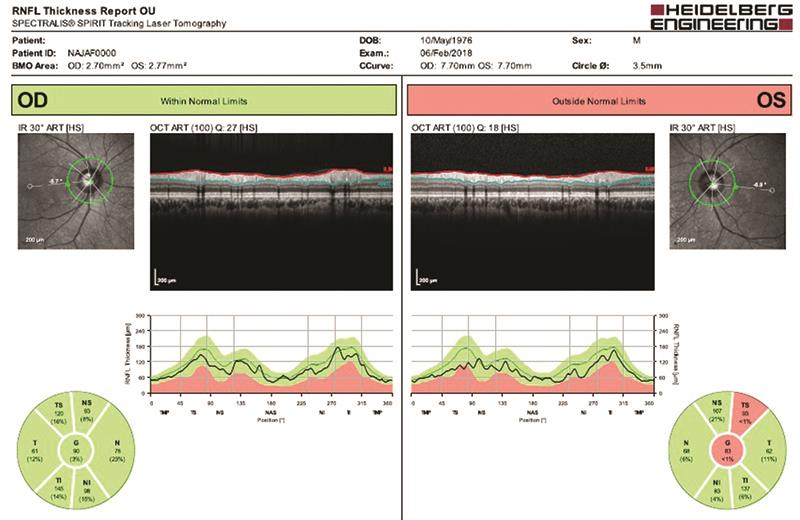
Figure 12
What has really won the argument for community OCT use has been the ability for accurate repeat use on patients over time to detect any change in structure. This, more than anything else, allows the instrument to detect disease sensitively. It is here that Heidelberg are able to win their spurs sensitively as monitoring patients requires accurate tracking.
One trick I have leaned over the years is to scan the same patient twice. In theory, with just minutes between scans, the values gained should be identical. Sadly, this is rarely the case with many instruments as focusing, patient movement and less than accurate tracking results in variation. Obviously, when seeing a patient and comparing the new values with those previously obtained introduces significant error in referrals.
The Spectralis Spirit includes the same TruTrack Active Eye Tracking patented technology as the Spectralis. This uses a second laser beam to actively track the eye during OCT scanning to avoid motion artefact. TruTrack effectively ‘freezes’ the retina, allowing you to capture the precise OCT image you want, even if the patient blinks or moves. It is widely accepted in hospital settings too, so any referral from the Spectralis Spirit based upon changes in values over any period will be taken seriously by hospital departments
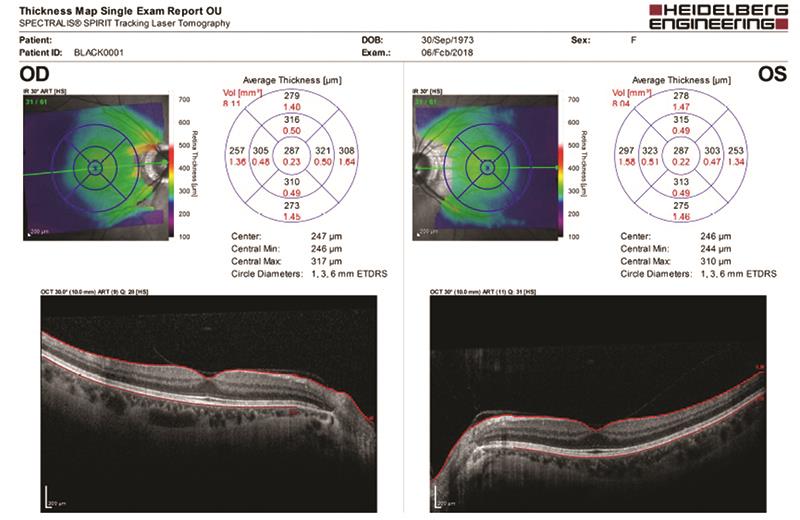
Figure 13
Patients
None of my sample of patients had concerns about their scanning and confirmed it was both quick and comfortable. Figures 13 and 14 show the results for a high myope and appear within normal limits for this sitting. Note how the scan around the disc clearly shows a still intact peripapillary vitreoretinal attachment.
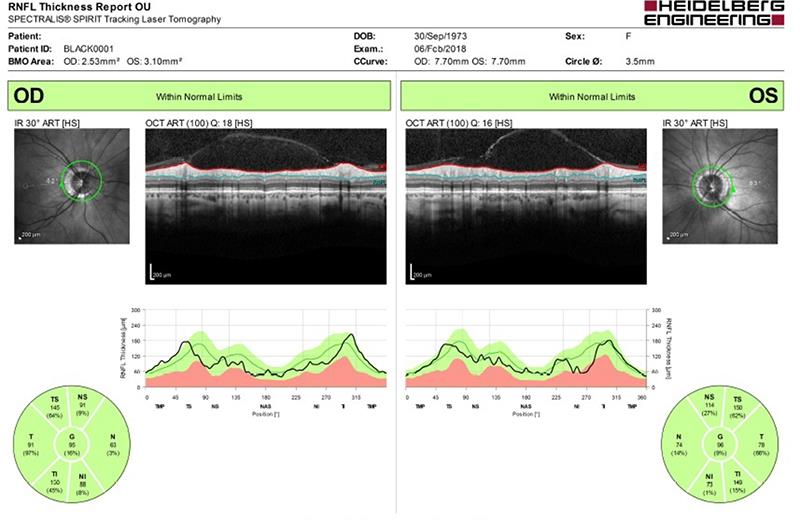
Figure 14
Finally, figures 15 and 16 show results from a patient showing some degree of suspicious retinal thinning and RNFL loss. He is being referred for this and, combined with full threshold fields, the results suggest there may well be glaucomatous neuropathy under way.
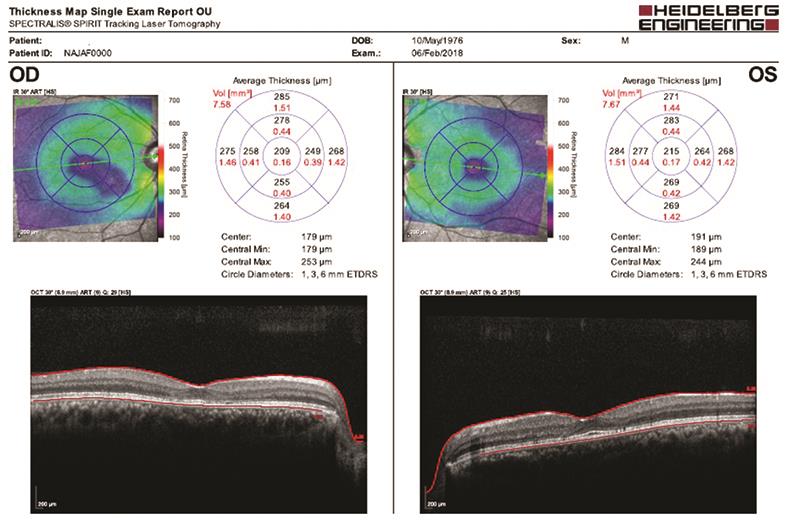
Figure 15
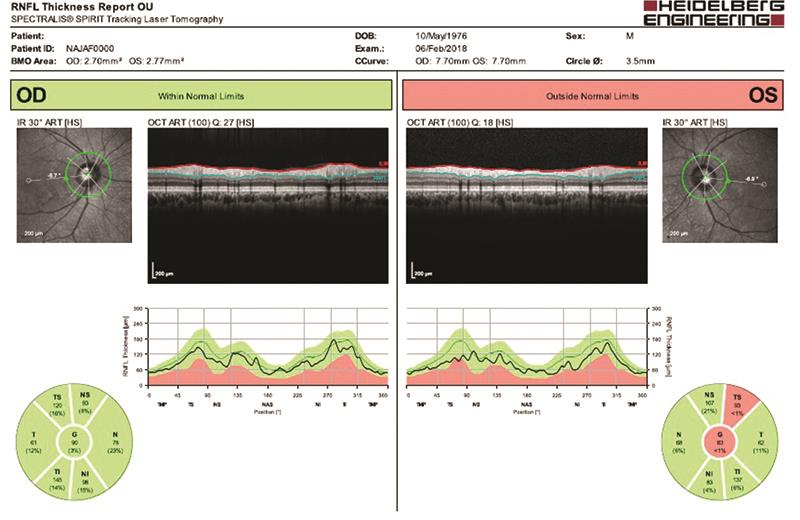
Figure 16
Easy Spirit
I believe the Heidelberg Spectralis Spirit is what the high street is waiting for – a reliable, easy to use OCT that allows useful scanning of ocular health in a way that most secondary care can relate to. The unit also allows further updates to anyone wishing to extend their OCT options.
For further information see www.LoveYourOCT.com