Sheraz Daya outlines a new approach to refractive surgery and describes his experience with the technique
IntraLase, the femtosecond laser in commercial use, is now available at Centre for Sight in the UK, one of only 166 of such lasers worldwide. It is futuristic technology that promises to revolutionise corneal surgery.
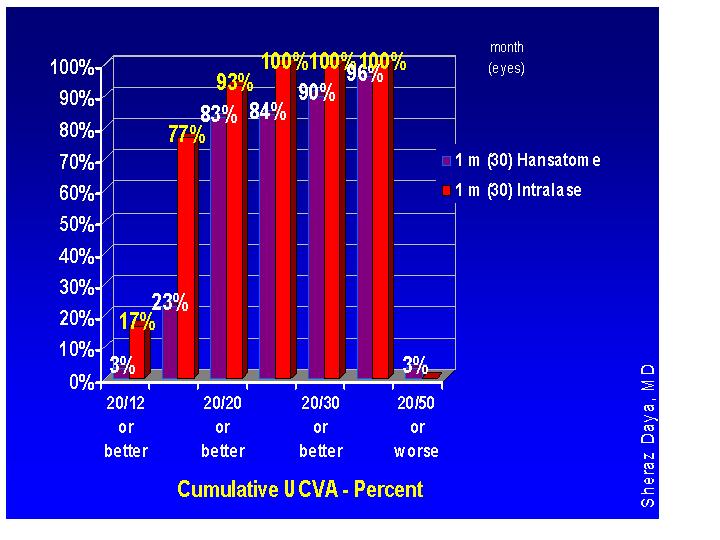
Figure 4. Keratome Lasik vs Intralase Lasik using same software (0 to -12.00D)
INTRACORNEAL RINGS
Intracorneal rings have been used for the correction of myopia and more recently there has been considerable interest in using this modality in keratoconus.4,5 While not always effective, it can delay corneal grafting by a reduction of both astigmatism and myopia enabling patients to tolerate contact lenses and spectacles again. Considering the relatively high incidence of keratoconus (1:2,000), this is a welcome option.
Problems with intracorneal rings have included infection, extrusion and induced astigmatism. These problems have resulted mainly from improper placement, with channels either too superficial or tilted (being deep at one end and superficial at the other). In the process of creating channels the cornea can also perforate.
The IntraLase laser has been used to insert rings and has the advantage of ensuring these are at uniform depth and accurately placed deep within the corneal stroma. The process of ring insertion is also more comfortable for the patient. The author has used the laser to create channels for insertion of rings and has found the process much easier (Figure 5). Whether there is a difference in refractive outcomes remains to be seen and is the subject of audit at Centre for Sight.
Register now to continue reading
Thank you for visiting Optician Online. Register now to access up to 10 news and opinion articles a month.
Register
Already have an account? Sign in here