It is such a great feeling to be able to make a positive change to someone’s life, and in this profession we are lucky enough to make this happen all of the time by giving people sight. Whether it be with spectacles, contact lenses, low vision aids or surgical procedures we help to change how these patients view the world. However, sometimes we need to help them by changing the way the world views them. So let us take a look into the life changing world of prosthetics.
What is a prosthetic?
A prosthetic by definition is a device, either external or implanted, that substitutes for or supplements a missing or defective part of the body. Depending on the condition of the eye the following can all be used as ocular prosthetic devices;
A full prosthetic eye or artificial eye – a type of craniofacial prosthesis that replaces an absent natural eye following eye removal. This might be subsequent to enucleation or evisceration. Enucleation is the removal of the eye that leaves the eye muscles and remaining orbital contents intact. Evisceration is a surgical technique by which all intraocular contents are removed while preserving the remaining scleral shell, extraocular muscle attachments, and surrounding orbital adnexa. The prosthesis fits over an orbital implant and under the eyelids. These are generally fitted by hospitals. They are made from either acrylic or glass, and are hand painted to provide the iris, pattern, pupil and scleral detail (figure 1).

Figure 1: A selection of prosthetic eyes
Facial prosthesis – following orbital exenteration (the removal of the entire contents of the eye socket, including eyeball, muscles, fat and tissues) a facial prosthesis can be supplied. These are constructed of acrylic and/or silicone rubber. They are positioned and held in place by adhesives or by attachment to spectacles, (figure 2).

Figure 2: Facial prosthesis from the front, left, and from above, right,. Photos courtesy of Anthony R Charman FBDO, Moorfields Eye Hospital
Cosmetic shells are moulded and hand painted and are generally manufactured in acrylic (figures 3 and 4). They can be made with an optical prescription can include a clear pupil and can provide a solution to ptosis. These can be fitted by optometrists or contact lens opticians in practice but are more commonly supplied by the Hospital Eye Service.

Figure 3: Cosmetic shells in close detail

Figure 4: Hand painting of a cosmetic shell
Prosthetic contact lenses are tinted, printed or painted contact lenses that are used to improve the appearance of a disfigured eye or to help correct the vision of a poorly functioning eye. A list of indications can be seen in table 1. They can be fitted in every day practice and can be made from a variety of materials (soft lens materials, RGP materials, PMMA). They may often be confused with a cosmetic lens which is a tinted, printed or painted lens used to enhance or alter the appearance of a normal eye. Note that the term ‘tinted lenses’ can be used to refer to both cosmetic and prosthetic contact lenses.1 Although optometrists and contact lens opticians may not always get a chance to fit these lenses, it is useful to know what is available for those occasions when a little bit of knowledge will make the world of difference to the patient.
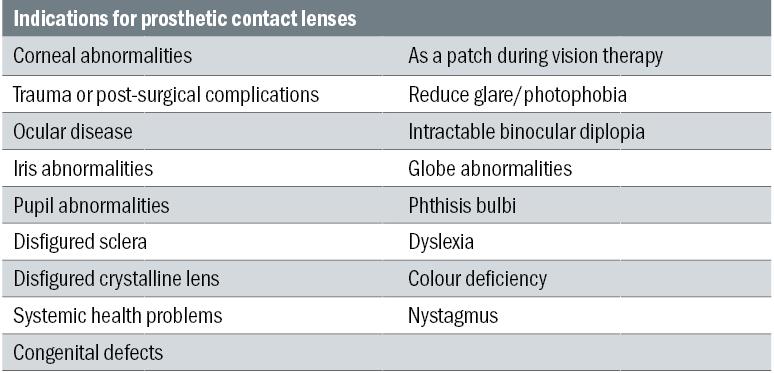
Table 1
Tinted prosthetic lenses
Most commonly made out of hydrophilic materials, people often think of these as a cosmetic lens to help to change the colour of the eye. When used as a prosthetic device they can help patients with photophobia which can be the result of various conditions such as achromatopsia, albinism or nystagmus. Tinted contact lenses have been reported to reduce photophobia and improve visual function in these patients as they act like sunglasses. Available in a wide range of materials including silicone hydrogel, the lenses can either just have a tinted iris with a clear pupil, can be tinted all over or solely have a tinted pupil (figure 5). Tint colour required can be down to patient preference and can be dependent on the patient’s condition, however, most patients will be happy with a brownish tint. Tinted contact lenses have also been used to assist with colour deficiency and conditions such as dyslexia. Cantor & Nissel Ltd and Cerium Group Ltd both supply a range of lenses suitable for these conditions, more information can be obtained from them directly.

Figure 5: A ChromaGen contact lens
Printed prosthetic lenses
Some contact lens manufacturers offer a soft contact lens which has an iris pattern printed onto the front surface. Different companies use different materials and different patterns, some of the moulded monthly or daily replacement lenses available are usually printed with a dot matrix pattern and are more commonly used as a cosmetic lens, although the pattern is sufficient to help disguise certain eye conditions. Iris and pupil diameters are often limited with these frequent replacement lenses, therefore more specialist lathe-cut options are more successful in covering a wider range of ocular conditions. These lenses are available with either a clear or black pupil and are available powered, making them an ideal choice for both sighted and non-sighted eyes. As the colours of printed lenses are pre-determined reproducibility is high, and the practitioner can use a colour chart to choose the closest match to the patient’s eye. Some manufacturers recommend that a pair of lenses are fitted to ensure an exact colour match between the eyes, however, consideration should be taken as to why the prosthetic lens is being fitted in the first place, if they only have one seeing eye the eye care professional may not want to risk fitting the seeing eye with a contact lens.
Hand-painted prosthetic lenses
Bespoke hand painted contact lenses can be fitted in everyday practice and offer improved cosmesis for many patients with an ocular abnormality. These used to be solely available in PMMA, but with advances in materials and paint availability hand painted RGP lenses were introduced and then more recently hand painted hydrogel lenses. HEMA was originally used, but nowadays high water content materials are favoured. Hand painted lenses ensure the exact pupil/iris diameter can be supplied. A larger range of lens diameters are available compared to printed lenses which mean that not only can the sclera be painted to mask abnormalities, but the iris/pupil can be painted off centre. This is particularly helpful for patients with a strabismus. Not only can the lens be painted to exactly match the colour of the good eye, but additional detail such as flecks, a naevus, pupil ruff, limbal ring, and (as already mentioned) scleral detail can also be added to provide an accurate match. Admittedly these lenses do take more chair time to fit when compared to printed lenses, however, the end result is worth it. With digital cameras to hand and, more commonly these days, smart phones being part of everyone’s lives, it is very easy to take a photo of the patient and email it to the supplier for a lens to be painted. Care must be taken to check that the patient gives consent for their photo to be shared with the supplier, and certain guidelines in health establishments such as hospitals should be adhered to. Even with that as a potential stumbling block, manufacturers have taken this into account and supply a more detailed colour match swatch.
Fitting soft prosthetic contact lenses
As mentioned above, this type of ocular prosthesis can be fitted in everyday practice and will help patients with many different conditions (see table 1). At the start of any consultation with a patient requiring a prosthetic lens, it is important to be both positive and realistic but without setting false hopes, getting the balance can be tricky for the optician. The patient needs to be aware that they are specialist lenses that cannot be bought ‘off the shelf’ and therefore attendance at multiple appointments will be required. Letting them know all costs involved is also a must at this stage, as most manufacturers do not offer a credit or exchange facility on such specialist lenses.
A decision needs to be made as to whether a tinted, printed or hand painted lens is required. This will be determined by the reason the patient needs the lens. Their iris colour can also play a part in making the choice. Patients with dark brown eyes are generally spoilt for choice as even a brown tinted lens would help to hide a small corneal disfigurement, as well as having the option of using a printed prosthetic lens or a hand painted lens. Patients with paler irises (such as blue, grey or green) will find that the best option will be printed or hand painted lenses as the tints are not usually dark enough to cover corneal opacities.
If the iris needs to be decentred on the finished lens or if any scleral detail is required then a hand painted lens will be the only option.
Once lens type is determined, it is best to consult the manufacturing lab for the lens information that they provide to ascertain what specific information and measurements are needed, along with the fitting procedure. Most manufacturing labs will also be more than happy to discuss which lens type they would suggest for the specific indications.
As with any contact lens trial, the patient should attend the consultation having had an eye examination within the past 12 months, if it was not done in the same practice then they should bring with them a valid and signed copy of their prescription. If fitting a sighted eye, the spectacle Rx (with back vertex distance if over +/- 4.00D) will need to be supplied. A full slit lamp examination should be carried out before moving on to the measurements.
Taking K readings may be tricky if the eye is damaged. In cases where they cannot be read it is advisable to base the measurements for the base curve on the other eye. Iris diameter should be measured. Once again the practitioner may want to base this measurement on the good eye. Although the vertical palpebral aperture is not necessarily used for the fitting of these lenses, it should be recorded and monitored for reference.
Pupil diameter should be measured in both low and bright illumination. The final pupil diameter ordered will be dictated by the patient’s occupation and daily lifestyle. If the pupil is blown or disfigured, measurements can be taken from the other eye. The manufacturer will need to know if a clear or black pupil is required.
Overall lens diameter required should be specified. A larger overall diameter may be necessary to ensure full coverage of the cornea. If the iris needs to be decentred on a hand painted lens then the amount of decentration needs to be taken into account.
It is likely that the lens manufacturer will suggest that a fitting lens is initially supplied from the measurements provided by the practitioner. This ensures that a good fit is achieved before expensive colours are added to the lens. Fitting lenses are either supplied clear or opaque and special stabilised fitting lenses will be provided when decentred or toric lenses are required.
Swatches are usually supplied by the manufacturer to help determine the lens colour required. If a tinted or printed prosthetic lens is to be used then photos are not usually needed, although they can be great to compare before and after shots. Ideally the patient should be taken to an area with good lighting, preferable natural light so that the natural iris colour can be seen. The practitioner can hold up the swatches provided to find the closest match, and this can be recorded for when the initial fitting has been completed. Even though swatches are still used for a hand painted lens, photos are also required to reference both the good and the bad eyes. The photo should be taken in good light between six to 12 inches away with a piece of white paper resting on the patients forehead, this is used by the artists to calibrate their computer screens to ensure the best colour match possible. If a swatch has been used, then this can also be held up in the photo. Giving the artist as much information to work with as possible, will ensure a more perfect match. It is advisable to take a picture of both eyes together as well as one of each of the eyes individually (figure 6).

Figure 6: Top: Ideal image for the manufacturing lab. Clear photo of both eyes the artist can zoom in to copy the fine details on the iris and sclera. Bottom: Although a closer photo of the eye, this is not clear enough to copy the detail
Even if the eye to be covered is completely opaque, knowledge of this for the artist is vital when deciding on what base colours to use. Digital cameras or smart phones are perfect for this job as the images can then be emailed straight to the lab. Though less common these days, and more often supplied by hospital photographic departments, labs are used to receiving good old-fashioned developed photos. The practitioner needs to conduct this process with sensitivity, a lot of patients are very conscious of their abnormalities and do not like having their photo taken, let alone it being sent for others to see. It is important to follow data protection guidelines at all times. The lab does not need to see all of the face, so a cropped pillar box image will be adequate and some patients will find this reassuring.
All of this information can now be supplied to the manufacturers and a fitting lens can be supplied.
Checking the fit of the fitting lens
At the start of the appointment it is worth reiterating that the lens you are about to try on the patient is solely for fitting purposes. A lot of patients at this point can become disheartened that the lens they have ordered is not there.
The lens should be inserted and allowed to settle. If it is being fitted to a seeing eye then the VAs should be checked and an over refraction performed and recorded.
The lens should be comfortable and should fit well. Centration and coverage should be noted. If the lens is not large enough or is not centring well it may be necessary to order a larger diameter. This will also be the case if the lens does not cover the abnormality adequately. As mentioned previously if any decentration of a painted iris is required the lens should be large enough to allow this.
If the lens has been supplied with an opaque iris or pupil, the size of these should be checked and any adjustments needed noted.
If any changes are required then it is advisable to order another trial lens and repeat the above.
Once happy with the fit and vision with the lens, the final lens can be ordered. The manufacturer may require the fitting lens to be returned to be tinted/painted, or they may be happy to supply a completely new lens. This will also depend on the lens type required as some lenses are printed in their dry state.
When the final lens has been made, the patient can now come in for a collection appointment. They will know what to feel comfort-wise and their expectations would not have been set too high in regards to appearance. However, this time they will have the bonus of having a more cosmetically pleasing appearance. The fit and vision should be checked with the lens and the lens colour should be assessed ideally in both indoor and outdoor illumination. A photo should be taken of the lens in situ for reference and this should be taken in the same place where the original photos were taken to ensure consistency. Printed lenses cannot be adjusted, tinted lenses can be made darker, and hand painted lenses can usually have slight adjustments made to them. A photo of both eyes should then be sent to the lab, even if no further adjustments need to be made it is great for them to see on eye the final lens (figure 7).

Figure 7: Before and after photo of Nissel Custom hand painted lens in situ (images courtesy of Angie Taylor, FBDO CL)
Aftercare
An insertion and removal appointment should be made and care instructions issued. Most prosthetic lenses are lathe cut, which means that they should last around 12 months. Some patients will find that they need to change them more frequently depending on wearing times and handling. It is important that the manufacturers recommended solution is supplied and that the patient is advised not to change brands unless it has been discussed with the practitioner. Certain care products can be contraindicated because of a particular ingredient or preservative, and use of the incorrect solution can accelerate fading. Patient education is of upmost importance in regards to handling of the lenses too.

Table 2
Even when following the correct care guidelines, some patients do find that their lenses will fade quicker than others. Obtain advice from the manufacturer as certain lenses can be re-opaqued. If this occurs it is a good idea for the patient to have two lenses on the go so that they are not without a lens when one has been sent away, though understandably some patients will not be too pleased with this idea when it comes to cost.
It is good practice to advise patients to wear spectacles over their prosthetic lenses. This can be for a number of reasons. Firstly from a safety point of view they can help protect the eye from injury. Secondly they can be used to improve appearance for the prosthetic eye, which can be beneficial if the prosthetic eye is smaller in appearance. Thirdly, they are not so commonly needed with the development of prosthetic lenses and better matches being available, but if the patient is conscious of their prosthetic lens, the spectacles can draw attention away from the look of the eye, and a tint can also be used to assist with this further.
An aftercare appointment should be booked and as long as care has been taken with all of the initial steps the patient should walk away very happy. And the practitioner can be satisfied that they have made a positive change to someone’s life.
Karen Hughes is a contact lens optician with a specialist interest in prosthetics.
References
1 Paulo Ricardo de Oliveira and Jeffrey J Walline. Cosmetic and Prosthetic Contact Lenses. Chapter 19. Contact lenses in Ophthalmic practice. Springer.