When dispensing complex or high powered lenses the following points must be considered:
? The prescription including the vertex distance
? Lens type, form and material
? Frame selection and fitting
? Field of view
? Spectacle magnification
? Centration
? Surface treatments
? The patient’s previous correction.
Vertex distance
Vertex distance is defined as ‘the distance from the corneal apex to the visual point on the lens’ and was discussed in Part 12. A vertex distance should accompany a spectacle prescription if the power of the lens in any meridian is ±5.00D and above, for example, -6.00/-1.00 x 50 at 14mm where ‘at 14mm’ refers to the vertex distance of the optometrist’s trial frame or phoropter.
Complex dispensing is often a balancing act resulting in a compromise somewhere along the line. Generally speaking, the prescription and inter-pupillary distance are items that cannot be changed. The power of the lenses ordered may of course differ from the optometrist’s prescription if there is a significant difference in the vertex distance of the spectacle frame and the trial frame/phoropter used during the refraction. The dispensing optician may choose to fit a spectacle frame with as short a vertex distance as possible in order, for example, to increase the field of view or reduce spectacle magnification. Other items that can be influenced by the dispensing optician include the lens material, centration, lens form, frame style, size, material and fitting. In many instances we have to play one off against the other, sacrificing frame size and zero decentration for higher refractive index materials or special lens forms. Whatever methods we employ, it is vital to try to imagine the finished result. This isan area in which computer-aided dispensing (along with a good relationship with your laboratory) comes into its own.
Frame selection, centration and decentration
The reasons for the correct centration of spectacles lenses are well known and include:
? The positioning of the zone of the lens where the paraxial prescription is most effective
? Reducing unwanted differential prismatic effects
? Reducing the possibility of the formation of ghost images.
Decentration is any displacement of the centration point from the standard optical centre position (boxed centre) and is necessary when the boxed centre distance of the frame and the subject’s inter-pupillary distance (or near centration distance in the case of a correction for near or intermediate vision) are not the same. Figure 1 illustrates the situation when the boxed centre distance of the frame and the subject’s inter-pupillary distance are equal, which of course means that decentration is not required.
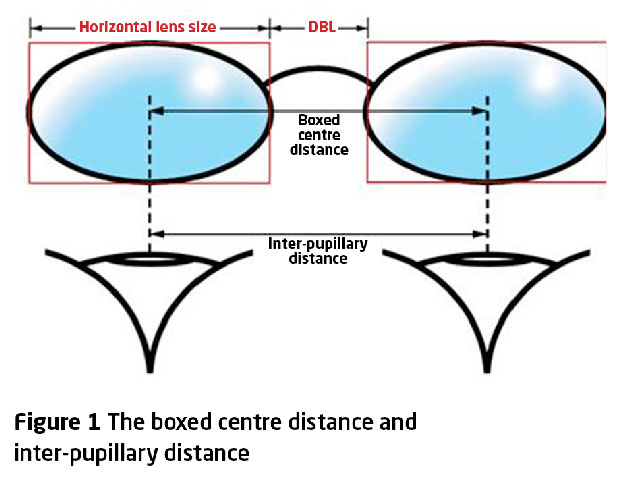
This is often thought of as being the ideal situation. Decentration can also be used to produce a given amount of prescribed prism. The effects of inward decentration on high-powered lenses are well known, with increased temporal edge thickness in minus lenses and increased nasal edge thickness in plus lenses (Figures 2 and 3).

Correct centration is of course important for all lenses and current international standards provide the required tolerances that we should be working to. However, the mechanical
consequences of decentration become more problematic when high-powered lenses are to be dispensed as the magnitude and direction of decentration can severely affect the thickness and appearance of the finished lens. As mentioned above, in order to keep horizontal decentration to a minimum, it is important to select a frame that has a boxed centre distance that is as close as possible to the required distance (or near/intermediate) centration distance.

This is particularly important when strong positive lenses are to be dispensed for near vision. We have all come across the situation when the nasal thickness of a lens is such that it is impossible to adjust the pad arms of a metal frame. The selection of a suitable frame is therefore a fundamental element of the dispensing process for both simple and complex prescriptions. This task is often delegated to less experienced practice personnel and initial errors in frame selection can result in problems if an alternative to the chosen frame has to be suggested for mechanical reasons. The most frequent problem encountered is when the frame selected requires excessive amounts of inward decentration to place the optical centres at the required centration points.
The previous prescription
When the practitioner is presented with a high-powered or complex prescription, it is essential that the practitioner takes a few minutes to examine the patient’s existing correction. Items of interest include:
? The refractive index of the lens
? Specific lens type and lens form
? Lens shape and size, aperture shape and size
? Vertical and horizontal centration
? Vertex distance, pantoscopic tilt and face-form angle
? Surface treatments
? Any special or unusual manufacturing techniques.
In order to avoid a non-tolerance to a new appliance it is often necessary to duplicate items such as lens form, lens material, centration and the general fit of a frame.
High myopia
Lens material and form
When faced with the task of dispensing strong minus lenses, three aspects immediately come to mind. These are:
? The selection of an appropriate lens material
? Special lenses for high myopia
? The selection of a suitable frame.
As far as lens selection is concerned, available products can be broadly divided into full-aperture lenses and reduced-aperture lenses.
The main mechanical consideration when dispensing strong minus lenses is the edge thickness of the finished lens. If the lens incorporates inward horizontal decentration the temporal edge will display the greatest edge substance. When dispensing full aperture lenses for medium to high myopic prescriptions the use of higher refractive index materials combined with aspherical surfaces and a reflection-free coating often provides the lens of choice. Such lenses give the practitioner a reasonable degree of control over the edge substance while providing good off-axis performance in oblique gaze.
All the major lens manufacturers produce resin materials with a consistent range of refractive indices, with the highest listed refractive index being 1.76. However, such products are invariably accompanied by lower Abbe numbers. Mineral (glass) lenses are available in refractive indices up to 1.9. Once again, such products often display low Abbe numbers, resulting in transverse chromatic aberration (TCA) and off-axis blur when the patient views through points away from the optical centre.
In order to keep effects of TCA to a minimum, the following points should be considered by practitioners. Use materials with a high Abbe number. Apply correct horizontal and vertical centration and pantoscopic tilt. Placing the optical centres of high-powered, low Abbe number lenses at the zero pupil position with a zero pantoscopic tilt will reduce the effects of TCA and hence avoid the possibility of reduced visual acuity in primary gaze. Be sensible with frame selection – consider shape and size carefully.
Fit the spectacle frame with as small a vertex distance as possible. The larger the vertex distance, the greater the distance from the optical centre to the visual point for a particular ocular rotation. So, fitting the lenses as close as possible to the eyes keeps the visual points as close to the optical centres as possible and minimises the effects of TCA. In addition, reducing the vertex distance will increase the field of view, reduce the spectacle magnification (minification) and provide a slight reduction in distortion. The application of a smaller vertex distance may also result in a lower-powered lens being ordered.
The weight of the finished lens is always a consideration when dispensing mineral lenses. This is because with mineral lenses, the density of the material (mass/volume) increases with refractive index. High refractive index glass (mineral) materials are heavier if we compare like with like – for example, a one-centimetre cube of one material with another of a higher density. However, when considering spectacles, this does not always result in a heavier finished lens. The reason for this is that a lens manufactured using a high refractive index glass (mineral) has less volume than a lens of the same power that has been manufactured using a normal refractive index material. In simple terms, there is less of it!
This means that even though the lens is made from a denser material its finished weight may be less than the same lens made using a normal refractive index glass material. In lower powers, however, it is probably correct to say that high refractive index glass lenses will be heavier. If weight is the patient’s priority then a resin lens has to be the material of choice. A reflection-free coating should always be applied to a higher refractive index material as ghost images 1, 3, 4 and 5 can be problematic to wearers of high-powered minus lenses.
A selection of products suitable for single-vision high-minus dispensing are listed in Table 1.

Most of the products in Table 1 are also available for the correction of hypermetropia. However, the plus end of the range is usually more restricted than the minus. For very high myopic prescriptions, a reduced aperture lens can be considered. Such lenses employ various techniques to reduce the edge thickness using smaller effective lens apertures while still maintaining a viable overall lens size for glazing (Figure 4a).

Reduced aperture lenses
Super Lenti (Norville)
The Super Lenti is a custom-manufactured series of blended lenses for high myopes which attempts to eliminate the obvious mechanical and cosmetic disadvantages of high minus lenses and is available in powers from -12.00D to -48.00D in glass and -12.00D to -22.00D in resin. Resin materials are available in refractive indices of 1.6, 1.67 and 1.74 and glass materials in refractive indices of 1.6, 1.7 and 1.8. The lens is decentred so that the optical centre is 4mm above the geometrical centre of the uncut, which is an advantage when it comes to frame selection. The lens should be fitted in the same way as a progressive power lens, so monocular centration distances and vertical centration must be specified. It should be noted that as the lens power and refractive index increases the diameter of the central aperture decreases. If the lens were glazed centred on the pupil, in the primary position, a zero pantoscopic tilt would be required. With higher powers, and therefore smaller apertures, it is best to fit with
zero pantoscopic tilt and as close to the eye as possible.
Benefits of this lens to the highly myopic patient include:
? Good visual acuity
? Good field of vision
? Controlled peripheral aberrations
? Good edge thickness and weight
? Allows for a wide range of frame selection
? Reasonable cosmesis
? Removal of the minification of the face which is seen with full aperture lenses.
Lentilux (Rodenstock)
The Lentilux is an aspherical, single-vision lens for the correction of myopia up to -24.00D. The stated advantages of this lens are:
? Good visual acuity
? Thin and light lenses. The edge thickness will not exceed 4.50mm even at -24.00D. The mean edge thickness for all powers is approximately 3.5mm
? Almost complete removal of power rings (ghost image no 1) due to the flat ‘rim area’ of the aspherical surface
? Removal of the minification of the face and distortion of the facial features, which is seen with full-aperture high minus lenses.
The back surface of the Lentilux is a rotationally symmetrical aspherical curve, both in the central and peripheral zones, which has been calculated by the lens designers to provide the optimum conditions for the wearer to achieve good visual acuity. The diameter of the central optical zone reduces by stages from 40-30mm as the power increases. For every 2.00D increase in power the diameter of the optically effective zone reduces by 2mm. The diameter of the optical zone of a -6.25D lens is 40mm, whereas for a -18.50D lens, the diameter is only 30mm. Rodenstock states that the field of view provided by the Lentilux is almost the same for all back vertex powers.
The outer circumference of the optical zone connects at all points to a ‘rim area’ in which the strong concave curvature of the power area continually decreases. It is this reduction in surface curvature that contributes to the considerable reduction in edge substance. The aspherical surface of the Lentilux has been optimised in the area surrounding the optical centre so that the patient is provided with the best possible off-axis acuity for a range of eye movements. A further thickness reduction is achieved by the fact that the lens is made using a high-refractive index glass material (Perfalux 1.7). Exact centration is important to avoid non-tolerances due to induced differential prismatic effects.
Lenticular lenses
When dispensing very high minus lenses a good cosmetic result can be achieved by the use of lenticular lenses along with careful dispensing and sensible frame selection. When compared to modern aspheric forms manufactured using very high index materials, lenticular lenses are often considered by some to be ‘old fashioned’. However, they still have a place in modern dispensing practice and minus lenticular forms are illustrated in Figures 4b to 4e.
Minus lenticular lenses are lenses in which the edge thickness has been reduced or ‘flattened’, resulting in an aperture and a margin. A line, similar to that of a solid bifocal usually exists between the flattened margin and the aperture. The aperture shape can be round, oval or profile with the margins usually being convex, plano or astigmatic in power. The major benefit of lenticular lenses is the reduction in volume and consequently a reduction in the weight of the finished lens.
The real field of view offered by minus lenticular lenses is also very good. Several manufacturers offer high minus lenses in lenticular forms. Zeiss, for example, offers high minus profile lenticular lenses in a choice of 1.5 and 1.7 glass materials or Clarlet 1.5. A profile lenticular is a reduced aperture lens where the shape of the aperture follows the shape of the lens. Depending on power, the optical aperture of profile lenticulars is usually 3 to 4mm from the lens edge. When dispensing profile lenticulars the frame should be chosen so that very little (if any) decentration is required.
Norville supplies minus lenticulars in a range of refractive indices in both glass and resin materials with powers up to -33.50D. Lentoid also offer a range of resin and glass lenticular lenses. The Norville range includes bi-concave aspheric and custom aperture lenticulars. Using free-from technology, Norville offers a process available on full-aperture lenses known as Slim Edge Technology (SET). This process, available with both plus and minus lenses, enables the reduction of lens substance by creating a blended edge effect.
With sensible frame selection, even extremely high powers can result in very neat and lightweight lenses, particularly if a profile aperture is chosen. To summarise, solutions for obtaining a cosmetically acceptable edge thickness in high minus powers are therefore:
? Little or no decentration
? Small horizontal and vertical eye sizes
? Very high index lenses
? The use of aspherical surfaces
? Specialist lenticular lens forms and edging techniques.
Thick edge substances can occur even when using very high index lenses and the frame chosen must be able to mechanically support such lenses. Frames manufactured using plastics materials and also thicker-rimmed metal frames provide good support and can help to obscure some of the edge thickness. Care should always be taken when selecting frames with adjustable pad bridges as excessive nasal edge thickness can obstruct the correct placement of the pad arms. Smaller eye sized frames with wider bridges and swept out lugs are ideal, as these help to reduce the required decentration and overall edge thickness while retaining a reasonable adult-sized head width in the frame.
It is well known that the real field of view obtained with a minus lens is greater than the apparent field of view. Even when reduced aperture lenses are used for the correction of high myopia the real field of view is still wider than the apparent field of view. It is interesting to note that a -15.00D lens dispensed with a 28mm aperture gives the same real field of view as a +5.00D lens with a 45mm aperture. Field of view will be considered in more detail in Part 15.
High hypermetropia
High-powered plus lenses present the practitioner with a different set of problems to overcome. Nasal edge thickness, centre thickness and overall weight are areas of most concern to both the practitioner and the patient.
Common problems associated with high plus powered lenses include:
? Weight and thickness of the finished lenses
? Oblique performance when viewing off axis
? Magnification
? Lack of accommodation if aphakic
? Restricted field of view
? Centration and prescribed prism.
Unlike high minus lenses, the finished blank size of a high-powered plus lens plays a vital role in dictating the final thickness of the lens when glazed. The avoidance of unwanted decentration is essential and by combining minimum substance surfacing techniques along with higher refractive index materials and aspherical surfaces, good results can be obtained (Figures 5a and 5b). Most major lens manufacturers offer a bespoke lens design service to help practitioners achieve good mechanical and cosmetic results and remote edging systems allow us to demonstrate these results to our patients in a matter of minutes without the need for complex calculations.

However, the use of aspheric lens forms when dispensing high plus lenses can dramatically improve the optical performance and cosmetic appearance of the finished lens. As an example, consider a +12.00DS lens made using spherical surfaces with a back surface power of -3.00D, centre thickness 10mm and a centre of rotation distance of 25mm. If an eye rotates 30° away from the optical axis of this the oblique power will be +12.00DS/+1.50DC. In other words, the refracted pencil will include +1.50D of unwanted cylinder. If the same lens were made using a convex prolate ellipsoidal surface (Figure 6) the off-axis performance would be +11.33D at 30°. The lens is now free from aberrational astigmatism. However, it is not an ideal design as the mean oblique error (MOE) at 30º will be -0.68D. Another improvement in the performance obtained by the use of a prolate ellipsoidal surface is a reduction in distortion as the distortion produced by the aspheric lens will be around 30 per cent less than in the spherical design.

Higher-order aspherical surfaces can be obtained by deforming a conicoid to obtain a surface which flexes back on itself at larger diameters (Figure 7). Such surfaces are known as polynomial surfaces. With polynomial designs the surface power reduces from the centre of the lens to the edge, where the periphery is afocal. These lenses usually perform well out to about 30º from the optical axis. The main advantage of this type of lens is the absence of ring scotoma and Jack-in-the-box effect which normally occurs at the edge of a strong plus lens. The lens therefore offers awareness of objects in the peripheral field. However the field of clear vision is quite small and wearers often turn their head to obtain a wide field of vision. These two effects are illustrated in Figure 8 and are due to the sudden change in power at the edge of the lens.
The advantages of polynomial designs are:
? No visible dividing line
? Good mean oblique power when viewing off-axis
? Reduced distortion
? Very slightly thinner
? Little sensitivity to fitting distance change
? Increased field of view
? Reduction in the ‘Jack-in-the-box effect’
? Flatter
? Less magnification
? Less TCA.
Although somewhat more restricted in availability when compared to minus lenses, plus lenticular lenses in various designs and apertures are still available. However, traditional lenticular lenses (Figure 9) for the correction of high hypermetropia have become far less popular since the introduction of polynomial designs. Norville provides an extensive range of plus lenticular lenses in various refractive indices and in powers up to +48.00D.
When dispensing high plus lenses, particularly for the spectacle correction of aphakia, there must be cooperation and communication between the prescriber and the dispensing optician to ensure that the trial lens prescription is reproduced as accurately as possible. Points that must be considered include:
? The form of the trial lenses used
? The pantoscopic angle of the trial frame
? The vertex distance of the trial frame.
It has been known for diligent optometrists to adjust and fit the chosen frame before the refraction takes place. The practitioner can then adjust the trial frame to match the characteristics of the final frame as opposed to the other way round!
As with high minus lenses, high plus lenses need to be mechanically supported by the frame. The position of the centre of gravity of a plus lens can often lead to the frame being ‘front heavy’ and prone to slipping. Regular fixed-pad bridge and saddle-bridge metal frames offer the best support and although adjustable-pad bridges allow the fit to be refined, excessive nasal edge thickness can obstruct correct placement of the pad arms and pads, resulting in poor fitting.
When dispensing high plus powers, frames selected should:
? Be lightweight to avoid heavy/thick rims adding to a ring scotoma
? Possess adjustable pads to allow some vertical movement of the optical centres
? Have a boxed centre distance as close as possible to the patient’s inter-pupillary distance in order to reduce or eliminate the need for decentration.
? Part 15 in the series will discuss dispensing for astigmatism and a selection of interesting freeform lenses.
Further reading
Fowler C and Latham Petre K. Spectacle Lenses: Theory and Practice, 2001; Butterworth Heinemann Oxford UK.
Jalie M. Principles of Ophthalmic Lenses 4th edition, 1984; The Association of British Dispensing Opticians London UK.
Jalie M. How to ensure the thinnest lens. Optometry Today, 2005; 22 April 28-36.
Jalie M. Ophthalmic Lenses & Dispensing 3rd Edition, 2008; Butterworth Heinemann Oxford UK.
Keirl A W. The properties of ophthalmic lens materials. Optometry in Practice, 2007; 8 4 123-138.
Keirl A W and Payne R J. Complex dispensing. Optometry Today, 2008; 48:04 28-39.
Norville Optical, 2012, Prescription Companion.
Ophthalmic Lens Availability, 2014. The Association of British Dispensing Opticians London UK.
Tunnacliffe A H. Essentials of Dispensing, 2003; 2nd Edition ABDO.
? Andrew Keirl is an optometrist and dispensing optician in private practice, associate lecturer in optometry at Plymouth University, ABDO principal examiner for professional conduct in ophthalmic dispensing, ABDO practical examiner and external examiner for ABDO College