It can be difficult for patients and practitioners to comprehend and compare the level of UV protection provided by different spectacle lenses due to usage of disparate measurement methods and associated nomenclature. Commercially available spectacle lenses claiming to provide ‘100%’ or ‘full’ UV protection refer to transmission, absorption, block, cut-off, UV400 and E-SPF, yet none of these terms have been consistently adopted to quantify UV protection.
Furthermore, use of ‘100%’ or ‘full’ to describe UV protection is also confusing; ISO 8980-3 define the UV spectrum as up to 380 nm, whereas the World Health Organisation (WHO) and the International Commission of Non-Ionizing Radiation Protection (ICNIRP) define UV radiation up to 400 nm, hence the development of UV400 lenses.
This article will explore the requirement for UV protection and the basis and limitations of current spectacle lens standards, as well as providing an overview of commercially available clear spectacle lenses claiming to provide UV protection.
What is UV radiation?
Ultraviolet radiation is high-energy, short wavelength radiation, which falls between X-rays and visible violet light in the electromagnetic spectrum. UV radiation can be subdivided according to wavelength into UVA (which ranges between 315 & 400 nm), UVB (which ranges between 280 & 315 nm) & UVC (which ranges between 100 & 280 nm).
UVC radiation from the sun is completely absorbed by the ozone layer and therefore does not reach Earth unless the ozone layer overhead has been damaged. A large proportion of UVB radiation is also absorbed by the ozone layer, whereas most UVA radiation from the sun is transmitted through the ozone layer and reaches us on the ground.
Multiple factors impact the level of exposure to UV radiation:
- Duration – the more time spent outdoors, the greater the exposure to UV. Indoor workers receive 10 to 20% of outdoor workers’ yearly UV radiation exposure.1
- Time of day – peak times for UV ocular exposure to the ocular surface are mid-morning and mid-afternoon, unlike for skin when noon is the peak time for exposure (when the sun is highest in the sky and the eyes are shaded by the brow).
- Latitude – UV radiation levels are higher the closer to the equator you are.
- Altitude – UV radiation levels are directly proportional to altitude, and for every 300 metres increase in altitude, UV increases by 4%.1 However, further from the equator the sun is lower in the sky for more of the day which can increase direct exposure of the ocular surface.
- Cloud cover – UV radiation levels are generally highest under cloudless skies, however, cloud cover has also been reported to increase the total UV radiation levels due to scattered or broken clouds acting as reflecting surfaces.2 Over 90% of UV radiation can penetrate light cloud.1
- Environment – different types of surfaces can reflect UV radiation: fresh snow can reflect up to 80%, dry beach sand about 15% and sea foam about 25%. At half a metre depth under water, UV radiation is still 40% as intense as at the surface. Shade can reduce UV radiation by 50% or more.1
- Driving – UV radiation is transmitted to varying degrees through different types of glass in car windows, although front windscreen protection is typically higher than side-window protection.3 An increase in prevalence of left-sided cataracts3 and skin cancers4,5 has been reported due to asymmetric UV exposure in drivers of left-hand-drive vehicles.
The impact of UV exposure
It is well understood that UV radiation can damage our skin; causing wrinkles, sunspots and skin cancers, however, many patients do not realise that UV exposure can also be harmful to the eyes and the surrounding skin. Children’s eyes are particularly susceptible to UV damage due to their bigger pupils and more sensitive tissue. However, research by the College of Optometrists found that 76% of parents in the UK do not protect their child’s eyes from the sun.6 The effects of overexposure to UV at a young age do not become apparent until later in life. A recent YouGov survey revealed that 54% of adults across Great Britain never, rarely or only sometimes wear UV protective sunglasses when they are outside in the sunshine.7 These statistics suggests a large proportion of the population are at risk of ocular UV damage.
Table 1 Summary of eye and eyelid conditions associated with chronic UV exposure
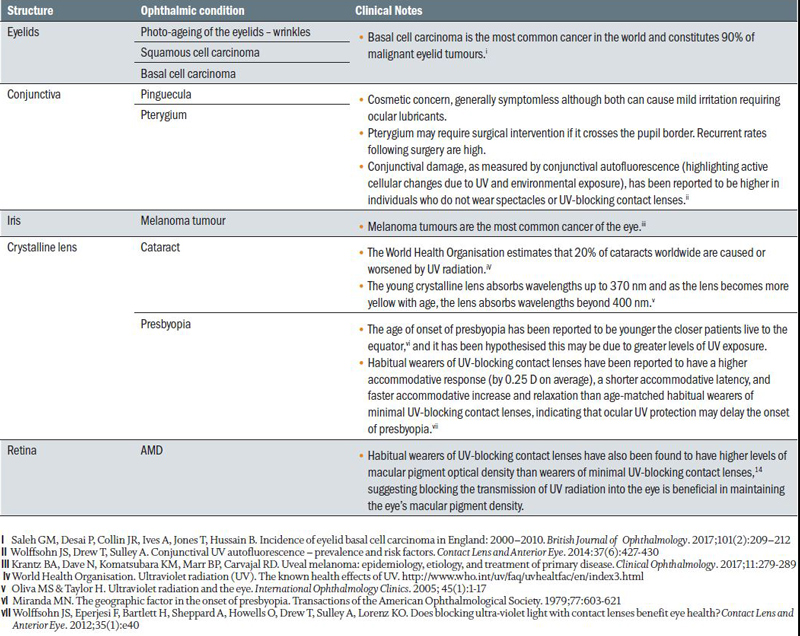
Short but intense UV exposure can cause acute damage, for example photokeratitis, whereas lower levels of exposure over a longer period of time can cause chronic damage. Chronic UV exposure can cause accelerated ageing of the skin around the eyes, and is implicated in the development of eye and eyelid conditions, summarised in table 1. While some patients may wear skin products, including eye creams, that claim to provide UV protection, it is unlikely these products are applied with sufficient frequency or thickness to protect the skin around the eye all day.
Spectacles can afford significant UV protection of the eye and surrounding skin, and accordingly eye care practitioners routinely recommend sunglasses for sunny days. However, UV protection is not only important on sunny days – we are all exposed to UV in winter as well as summer, even in overcast conditions. While people do not typically wear sunglasses on cloudy, overcast days, it is estimated that nearly 70% of the UK population wear prescription glasses to help them see; representing a significant opportunity to provide ocular UV protection in clear lenses for a large proportion of the population.
Spectacle lens standards for UV protection: 380 nm versus 400 nm
Although the WHO and the ICNIRP define UV radiation hazard extending up to 400 nm, both the International Standards Organisation (ISO) and the American National Standards Institute (ANSI)8 have chosen to disregard the wavelength range between 380 and 400 nm. The latest Australian and New Zealand sunglass standard9 considers UV radiation up to 400 nm, however international clear lens standards are yet to adopt this approach. The rationale behind this decision is unclear, and creates ambiguity over the meaning of the commonly used marketing claims ‘full UV protection’ and ‘100% UV protection’.
Twenty extra nanometres may not seem significant, but to understand the importance of the cut-off value for UV protection, it is necessary to consider the level of spectral irradiance and the ocular hazard posed.
Figure 1 Relative irradiance as measured on Earth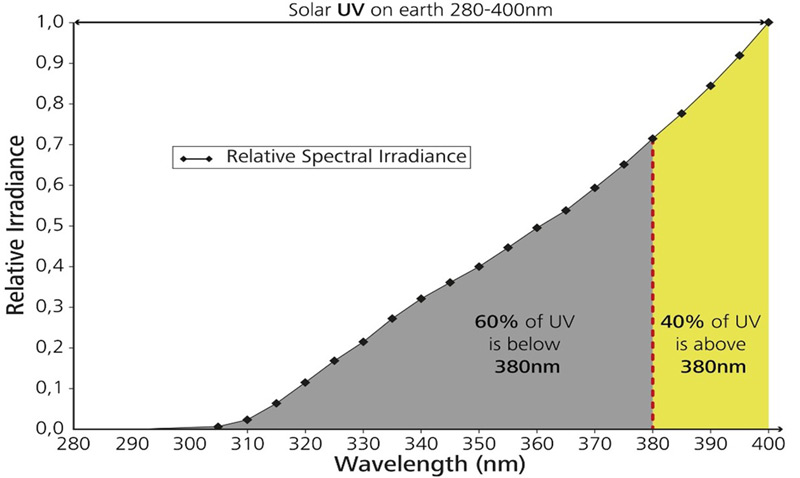
UV radiation between 380 and 400 nm accounts for almost 40% of the total amount of solar UV irradiance as measured on Earth10 (figure 1). UV rays with shorter wavelengths may have higher energy levels, but radiation between 380 to 400 nm penetrates tissue more deeply (figure 2).
Figure 2 Longer wavelength UV radiation penetrates deeper into the
skin, damaging skin cells and causing photo-ageing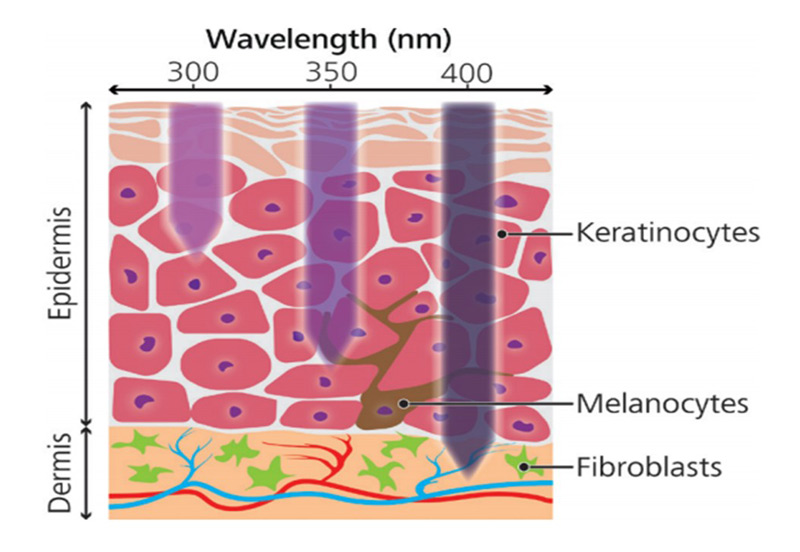
The ocular hazard can be determined by weighting each wavelength according to its ability to cause a specific type of damage to a specific tissue. As discussed in the previous section, there are multiple sites and mechanisms for UV damage in the eye. Clear ophthalmic lenses standard ISO 8980-3 has adopted the commonly used spectral weighting function published by ICNIRP,11 considering UV exposure to the ocular surface, with reduced hazard as the wavelength gets longer (figure 3). However, the CIE photocarcinogensis action spectrum weights wavelengths from 380 to 400 nm the same as wavelengths between 350 to 380 nm.12 Additionally, recent research investigating UV exposure of keratinocytes (cells producing keratin) and fibroblasts (cells producing collagen and other fibres) suggest a much larger threat from wavelengths longer than 380 nm (figure 3).13
Figure 3 Relative hazard for ISO 8980-3 according to wavelength
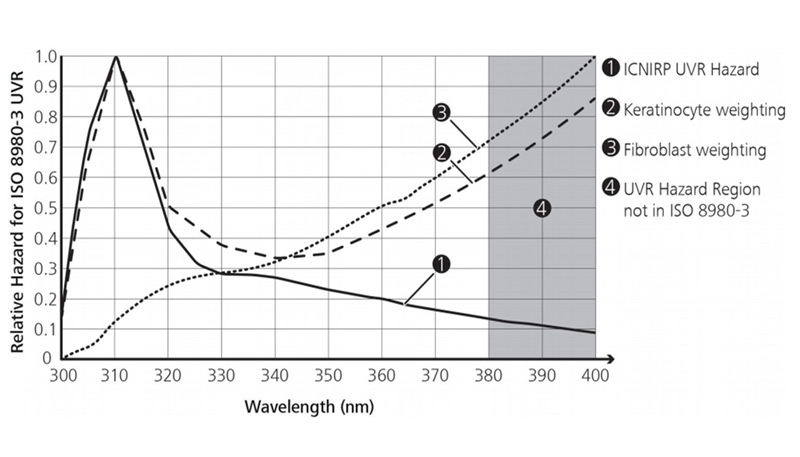
Therefore, it seems likely that current standards have underestimated the physiological impact of UV radiation between 380 to 400 nm, and that UV protection up to 400 nm should be recommended for all patients.
UV protection challenges for spectacle lenses
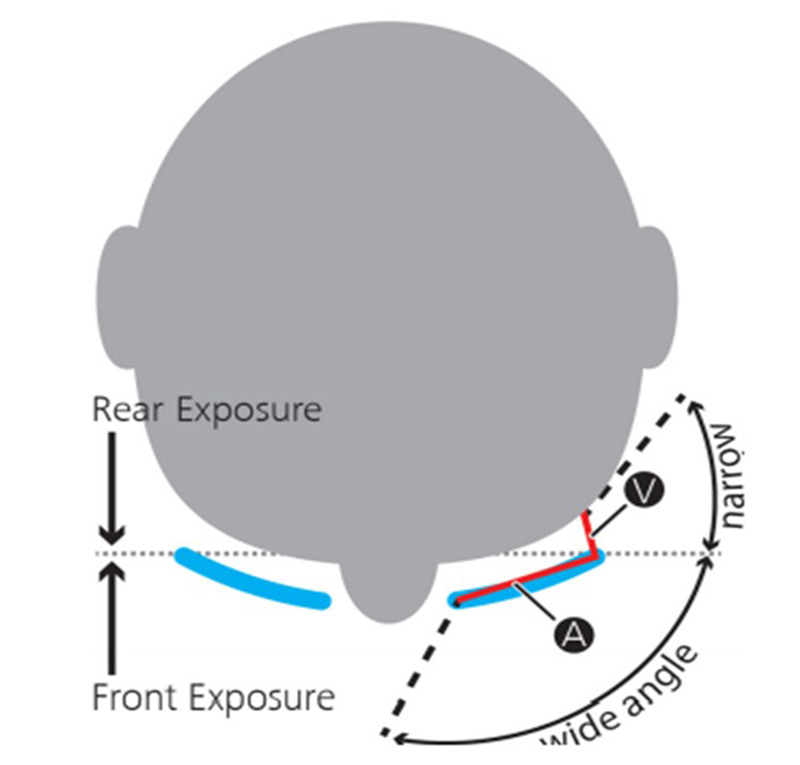
Spectacles can provide significant eye and eyelid protection from UV radiation. However, spectacle lens manufacturers face multiple UV protection challenges; direct UV radiation incident through the front of the lens, indirect UV radiation entering from the sides and rearward reflections from the back surface of the lens. The proportion of UV radiation reaching the eye from each route can be determined by considering the angular expanse of the source and the area of the aperture.14 For spectacle lens wearers, the rearward entry angle and aperture (labelled V in figure 4) are much narrower than the forward angle and aperture (labelled A in figure 4). Accordingly, approximately 90% of the incident UV radiation comes through the front of the spectacle lens. A small proportion of UV radiation is reflected towards the eye from the back surface of the lens. However, it is worth noting that not all rearward UV radiation is reflected off the back surface of the lens, as some passes straight through the lens from the back to the front surface and therefore does not reach the eye.
In order to resolve the key ocular UV protection challenges spectacle lens wearers face, it is necessary for lens manufacturers to consider both the direct UV radiation incident through the front of the lens, and the rearward reflected UV radiation. Lens manufacturers have taken two approaches to tackle these challenges:
1 Integrating a UV absorber into the clear lens substrate.
2 Applying an enhanced back surface anti-reflective coating.
Clear lens substrates
Eye care practitioners will be aware that some lens materials inherently absorb a proportion of UV radiation, as shown in figure 5. Polycarbonate lenses absorb UV radiation up to 380 nm, and therefore according to ISO 8980-3 definition of UV radiation (up to 380 nm), provide ‘full’ UV protection. As a result, some lens manufacturers have overlooked the importance of UV radiation incident through the front of the lens. However, as discussed in a previous section, protection up to 400 nm is recommended and consequently UV radiation incident through the front of the lens is an important consideration in the development of spectacle lens UV protection.
Standard 1.5 refractive index lenses provide UV protection up to 355 nm, however, the wavelengths between 355 and 400 nm represent about 70% of the total amount of solar UV irradiance.15 Standard 1.5 refractive index lenses account for approximately 50% of the lenses sold globally,15 and even higher index materials do not provide maximum UV protection up to 400 nm, suggesting most spectacle lens-wearers are at risk of chronic ocular UV damage.
It is challenging for lens manufacturers to incorporate UV absorbers into clear lens materials to provide UV protection up to 400 nm without introducing a significant hue that compromises the cosmetic appearance and visual performance of the lens. With Zeiss UVProtect lenses, Carl Zeiss Vision have incorporated UV absorbers into clear lens polymers, providing UV protection up to 400 nm in all clear plastic lenses, as shown in figure 5, without noticeably changing visible light transmission. Competitors are yet to integrate equivalent UV absorbers into their lens materials, and have instead focused on reducing the reflections from the back surface of the lens with back surface anti-reflective coatings.
Figure 4 Schematic representation depicting entry angle and aperture,
where A denotes the area of the spectacle lens and V denotes the area
of gap between the frame side and spectacle lens wearer’s head
Back surface anti-reflective coatings
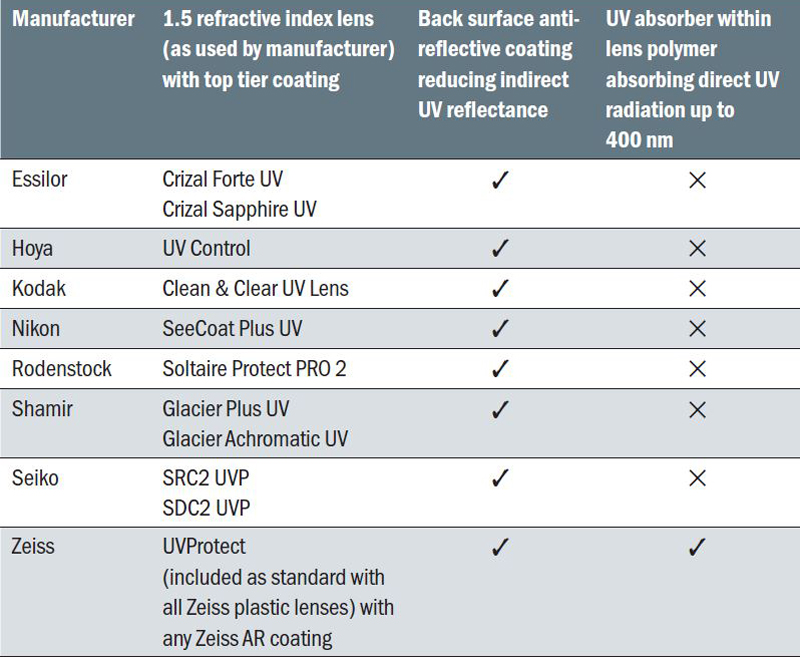
Most lens manufacturers now offer lens options with enhanced back surface anti-reflective coatings, incorporating additional layers to significantly reduce UV radiation reflected into the eye from the back surface of the lens. While the products listed in table 2 may reduce reflected UV radiation up to 400 nm, in isolation, back surface anti-reflective coatings do not provide any protection from the UV radiation incident through the front surface of the lens, which as discussed earlier, represents approximately 90% of the UV radiation reaching the eye. Therefore, as you would expect, significantly more UV radiation reaches the eye when wearing lenses incorporating only an enhanced back surface anti-reflective coating when compared to wearing lenses also incorporating a UV absorber within the lens substrate. Such back surface anti-reflective coatings could even increase the transmittance of direct UV radiation incident through the front of the lens, just like a visible light anti-reflective coating increases transmittance of visible light.16
Figure 5 Relative spectral transmission of standard lens materials and
Zeiss UVProtect lenses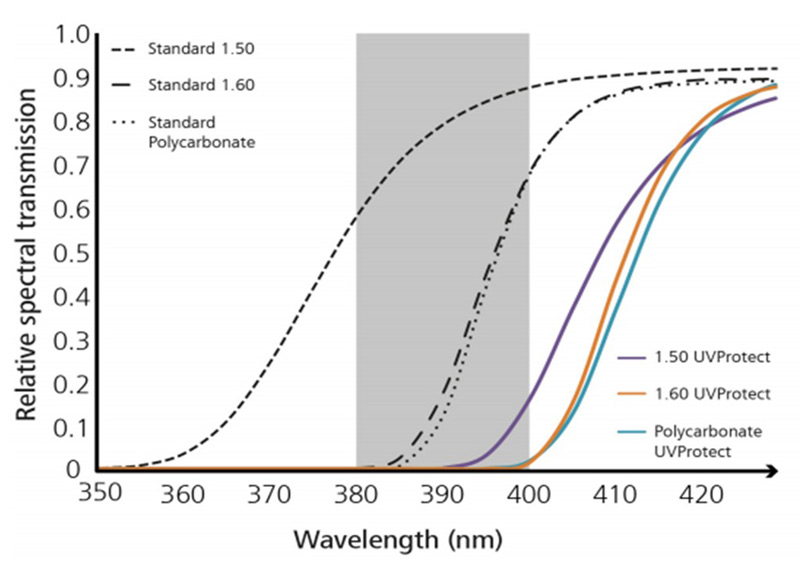
Summary
UV radiation from the sun is always present and it is important that eye care practitioners educate patients and recommend lenses providing protection from the chronic effects of UV exposure. Current international standards truncate the range of UV radiation and do not necessitate UV protection up to 400 nm, however the spectral range between 380 to 400 nm is plentiful and harmful to ocular tissue. Most clear spectacle lenses fall short of fully protecting patients’ eyes from UV radiation. Spectacle lenses incorporating a UV absorber and an enhanced back surface anti-reflective coating provide the best protection from UV radiation up to 400 nm.
Table 2 Summary of commercially available clear refractive index 1.5
plastic lens products in the UK claiming to provide UV protection
Clinical recommendations
To protect patients from chronic ocular damage due to UV exposure, recommend spectacle lenses providing UV protection up to 400 nm for all clear spectacle lens wearers and all sunglass wearers, especially important for patients with outdoor occupations and hobbies.
The degree of protection afforded by spectacles depends on multiple factors including lens size, back vertex distance and lens material, so it is important that frame selection is guided and all spectacles are fitted by a professional in practice.
While clear spectacle lenses providing UV protection up to 400 nm are recommended for general use, sunglasses (also providing UV protection up to 400 nm) should still be worn on sunny days to reduce glare and provide visual comfort and clarity.
Dr Debbie Laughton is Head of Professional Services and Paul Hopkins is Professional Services Associate, Vision Care Business Group, Carl Zeiss Vision UK Ltd. Professor James Wolffsohn is Associate Pro-Vice Chancellor at Aston University.
References
- World Health Organisation. Global Solar UV Index: A Practical Guide. 2002. http://www.who.int/uv/publications/en/UVIGuide.pdf
- Lubin D & Frederick JE. The ultraviolet radiation environment of the Antarctic Peninsula: The roles of ozone and cloud cover. Journal of Applied Meteorology. 1991;30:478-493
- Boxer Wachler BS. Assessment of Levels of Ultraviolet A light protection in automobile windshields and side windows. JAMA Ophthalmology. 2016;134(7):772-775
- Chang C, Murzaku EC, Penn L, Abbasi NR. Davis PD, Berwick M, Polsky D. More skin, more sun, more tan, more melanoma. American Journal of Public Health. 2014;104(11):e92-e99
- Fosko SW. Left-sided skin cancer: Importance of age, gender, body site, and tumor subtype in studying skin cancer laterality and implications for future research and public health interventions. Journal of the American Academy of Dermatology. 2011:65(1);208-210
- College of Optometrists Survey August 2009. Parents risk their children’s eyesight in the sun. http://www.college-optometrists.org/en/knowledge-centre/news/index.cfm/parents_risk_their_childrens_eyesight_in_the_sun
- YouGov Plc Survey July 2018. https://www.fightforsight.org.uk/news-and-views/articles/news/research-shows-one-in-two-brits-putting-eye-health-at-risk-during-sunny-weather/
- ANSI Z80.1-2015 Ophthalmics - Prescription Ophthalmic Lenses Recommendations. American National Standards Institute
- AS/NZS 1067:2003. Australian / New Zealand Standard. Sunglasses and fashion spectacles
- Mecherikunnel AT & Richmond JC. NASA Technical Memorandum 82021. Spectral Distribution of Solar Radiation. 1980. https://ntrs.nasa.gov/search.jsp?R=19810016493
- International Commission on Non-Ionizing Radiation Protections; Health Physics. 2004;87(2):171-186
- ISO/CIE 28077:2016(E) Photocarcinogenesis action spectrum (non-melanoma skin cancers)
- Latimer JA, Lloyd JJ, Diffey BL, Matts PJ, Birch-Machin MA. Determination of the action spectrum of UVR-induced mitochondrial DNA damage in human skin cells. Journal of Investigative Dermatology 2015:135.10:2512-2518
- Rifai K, Hornauer M, Buechinger R, Schoen R, Barraza-Bernal M, Habtegiorgis S, Glasenapp C, Wahl S, Mappes T. Efficiency of ocular UV protection by clear lens solutions. Biomedical Optics Express. 2018;9(4):1948-1963
- Share of 1.5, Mid-Index & Polycarbonate lenses. World lens and frame demand study 2016. Strategy with Vision
- ZEISS data on file.