Conventional cigarettes use does appear to be falling. However, since their introduction in 2003, e-cigarettes are giving concern to a range of clinicians. There appears to be two schools of thought: one of harm minimisation, with considerable support from national organisations, such as Public Health England (PHE), that insist that e-cigarettes are ‘at least 95% safer than cigarettes’1; the other is more precautionary and supported by the European Respiratory Society2 and the Federation of International Respiratory Societies3 among others,4 coming out strongly against their use. Additionally, there is disagreement on the potential impact on adolescents, creating a further global divide on policy.5
Figure 1: The impact of nicotine addiction, particularly in the young, cannot be underestimated

E-cigarettes deliver nicotine by vaporising propylene glycol/vegetable glycerine, nicotine, and flavourings.6 The nicotine hit induces pleasure, reduces stress and anxiety, and causes addiction.7 E-cigarette technology and designs have evolved8 and have been the subject of a growing body of research focused on the chemical makeup and risk analysis of chemicals, metals, and particulates found in e-cigarette liquids and vapor.
In this article I address the following question: Are e-cigarettes the health benefit that their supporters suggest, or an emerging and sinister threat to health?9,10
Harm Reduction?
How safe are e-cigarettes? The fact they do not produce either tar or carbon monoxide is better than cigarette smoke.9 There is, however, growing evidence of their health risks,11 coupled to the fact they contain nicotine, an addictive drug.12
Figure 2: An early cigarette-like e-cigarette

The dangers of nicotine exposure among the young has been highlighted in a recent US Surgeon General advisory document (2018) where nicotine exposure during adolescence can impact learning, memory and attention, and brain development.13,14,15
Nicotine exposure from e-cigarettes is not the only concern. There are thousands of different combinations of compounds and flavourings that can be vaped. Very few of have been studied and regulation is limited. Those that have appear to have their own adverse effects and should not be considered watered down versions of tobacco.16 Some studies found vape liquids contained substances that have some level of hazard/risk of danger17 and breech the European Tobacco Products Directive (ETPD) , prohibiting the addition of compounds which pose a risk to human health, either when heated or not (only nicotine is excepted).18
Vape fluids have different effects to those of tobacco smoke on lung tissue and specifically cause marked biological changes to the bronchial epithelium.6 These changes are not harmless and are linked to the development of chronic obstructive pulmonary disease (COPD),6 as well as having an association with myocardial infarction.11
Those in favour of a more liberal regulatory approach on vaping acknowledge that the long-term safety of this addiction is not known. This is concerning given that the effects of second hand tobacco smoke are still emerging, taking decades to manifest.9 An example of this is a recent study where an increased risk of death from COPD was found in non-smoking adults who were exposed to second hand tobacco smoke in childhood.19 The discovery of these associations after many decades of being exposed to second hand tobacco smoke means that it will be very many years before we can determine whether passive exposure to vaping is safe.9 Indeed, although research is limited, the evidence is that second hand exposure to vaping emissions is not safe.20,21,22
There is particular concern about the now widely cited claim by Public Health England (PHE) that e-cigarettes are ‘95% safer’ than traditional cigarettes. This figure is based not on empirical data but on a meeting of individuals, whose report conceded that the evidence was insufficient to reach a robust conclusion.23 The PHE’s view is far from universally accepted in the UK,24 where the National Institute for Health and Clinical Excellence (NICE), which evaluates evidence on effectiveness of treatments, does not recommend them as cessation aids.25 The claim is also viewed with scepticism abroad,26 with concerns expressed of this apparent ‘evidence-deficient’ endorsement27 determining public policy in the UK.24 Some toxicologists consider the Public Health England’s promotion of e-cigarettes as ‘a reckless and irresponsible decision’,28 and some respiratory experts express concerns that continuing with the current PHE approach risks ‘a further epidemic of devastating lung disease for today’s children.’9
Gateway or Road Block?
There is a marked difference of opinion regarding whether the use of e-cigarettes by young people serves as a gateway to tobacco smoking rather than a means of cessation.9 Recent reports from the UK29 and USA30 highlight these opposing views. The US report cites ‘there is substantial evidence’ of a gateway effect, whereas the UK report concludes ‘e-cigarettes are attracting very few young people who have never smoked into regular use.’
Looking at the literature, the argument against a gateway runs that vaping has been rising while smoking continues to fall.31 So, vaping cannot be causing any significant degree of increased harmful smoking among adolescents.32 In truth, declining trends of smoking among youth were apparent well before the introduction of e-cigarettes.33,34 A recent study that analysed data from nine clinical trials, taking into account a variety of risk factors, concluded that the odds of subsequent cigarette smoking by non-smokers who had any experience of vaping more than tripled compared with those with no vaping experience.35
Those who do not support the gateway effect suggest that people switching from e-cigarettes to traditional tobacco share common risk factors.31 Interestingly, several longitudinal studies have reported the strongest association between e-cigarette use and smoking initiation among youth with the lowest risk of smoking.36,37 More concerning are studies that show that a third of youth who start with e-cigarettes have risk profiles that make them unlikely to start with cigarettes.38 Another argument supporting vaping often put forward concerns the a natural propensity for some people to smoke; or, to put it another way, ‘kids who will smoke, will smoke’. If this were true, how then do we explain the dramatic falls in uptake that have been seen in countries that have robust, comprehensive tobacco control programmes?
Critics of the idea that there is a gateway effect also state that studies proving a gateway effect often fail to discriminate between experimentation and regular use, and some researchers question whether a single puff or occasional e-cigarette use can lead to regular smoking.39 In reality, every regular smoker started with a ‘simple puff,’ nearly always in their youth,38 typically progressing through more regular use to daily smoking. It has been recently reported that over two-thirds of smokers who tried as little as a single puff became, for a time, regular smokers.40
Nicotine
The impact of nicotine addiction, particularly in the young, cannot be underestimated (figure 1). A ‘sleeper effect’ exists, whereby initial exposure to nicotine lead to a vulnerability to future smoking for three or more subsequent years.41 The ‘neurobiological insult’ of nicotine was recently highlighted in the US Surgeon General’s report on the potential risks of nicotine and electronic cigarettes to youth.42 Indeed, this stated that ‘The first symptoms of nicotine dependence can appear within days to weeks of the onset of occasional use, often before the onset of daily smoking.’43
Figure 3: Tank-style e-cigarette

There does not appear to be a minimum nicotine dose or duration of use as a prerequisite for symptoms to appear.44 In some cases, even smoking on a monthly basis greatly increases the likelihood of developing dependence in a younger person.45 In keeping with the theme of addiction, the US Surgeon General raised the concern that nicotine in adolescence can also increase the risk of future addiction to other drugs.15 Bearing this in mind, it is alarming that e-cigarettes are becoming a known, viable, illicit drug delivery system. Some studies, citing survey respondents, found more than a third were actively using their vaping device to inhale recreational drugs.15,46
Given the addictive potential of nicotine, it is worrying that a reported 90% of vape shops are selling products to adults who have never smoked or vaped, and therefore breaching the code of conduct that applies to these businesses.47
There is growing evidence that, for many young people, the first contact with nicotine is in the form of e-cigarettes48 and that their use is strongly associated with a subsequent progression to tobacco products.49 Some clinicians feel that the debate around ‘safety or gateway’ misses the fundamental question of whether it is desirable that young people should be exposed to nicotine, a known drug of addiction, at all. They instead advocate stressing the need to get across the message that nicotine is a dangerous drug of addiction, and that young people must be warned of the adverse consequences, and protected as far as possible therefrom.9 Some suggest adopting regulations that apply to tobacco should be applied to e-cigarettes, including those relating to advertising, packaging and taxation, where possible. The only justification for their use is when aligned with nicotine patches and gum for the specific purpose of smoking cessation.9
Cessation
Does the use of e-cigarettes help adult smokers give up conventional tobacco products? Research into the concentration of nicotine deliverable in e-cigarettes does suggest that, for adult smokers trying to stop, e-cigarettes can be an effective tool.50,51,52
Figure 4: The JUUL showing main unit (left) and the JUULpod which contains the e-liquid and serves as a mouthpiece

Adapting the speed of nicotine delivery from e-cigarettes may assist smokers in fully switching away from conventional cigarettes53 Other nicotine replacement therapies (NRTs), such as nicotine gums, patches and inhalators, deliver nicotine much more slowly and at lower doses than conventional cigarettes.54
The form of nicotine used plays an important role. Conventional e-liquid – termed freebase nicotine – is more volatile and likely to be deposited in the oral cavity/upper respiratory tract. This results in a slower absorption profile, more closely resembling that of an NRT than that of a conventional cigarette.55
The need for more effective and appealing e-cigarette products, to provide satisfying alternatives to smoking, has led to the recent development and marketing of e-liquids containing nicotine salts. Nicotine salts are formed by the reaction of nicotine with a suitable acid and are less volatile than freebase nicotine.56 More of the nicotine (in salt form) reaches the alveoli of the lung for pulmonary absorption, replicating a cigarette-like nicotine delivery in the lung. The implication is that nicotine salt inhalation devices should enable the adult smoker to get the same nicotine ‘hit’ and therefore make them more appealing products for adult smokers who are switching from cigarettes to vapour products. This is in line with public health recommendations in the UK.51
The e-cigarette active ingredient concentration generally advocated is 40mg nicotine lactate, which has the closest nicotine uptake profile to that of a conventional cigarette, resulting in greater user satisfaction and less desire to continue to smoke as before. However, this concentration of product would not be permitted in the European Union. Both Public Health England and the Royal College of Physicians have stated that the cap on nicotine concentrations imposed by the ETPD may limit the effectiveness of e-cigarettes as a smoking substitute, particularly for heavier smokers.57,58
Increasing the nicotine strength of liquids with nicotine lactate formulations and suitable flavour options that can be legally marketed to smokers may maximise the public health potential of e-cigarettes.50
Evidence of Effectiveness
Once again there is no general policy consensus regarding the effectiveness of e-cigarettes in smoking cessation. A recent US report states ‘there is insufficient evidence from randomized controlled trials about the effectiveness of e-cigarettes as cessation aids compared with no treatment or other smoking cessation treatments.’3 The view of PHE is to recommend that ‘e-cigarette use, alone or in combination with licensed medication and behavioural support from a Stop Smoking Service, appears to be helpful in the short term.’29
The rationale that e-cigarettes have the potential to increase cessation rates is not necessarily backed up clinically, with much of the available evidence actually suggesting a reduction in cessation rates.59 Where evidence does exist, it is not convincing,60 and indeed in a recent trial, paying people to stop smoking was the only effective strategy.61 A meta-analysis actually revealed that e-cigarettes were associated with less quitting among smokers.62
Commercial Pressures
It is accepted that NRT plays an important role in tobacco cessation, especially when combined with counselling.63 ‘Big tobacco’ – corporations that profit from the sale of tobacco – has had an interest in NRT for many decades, adopting the approach that suggests ‘if anyone is going to take away our business it should be us.’64 On the other hand, many health practitioners, researchers, and policy makers instead view e-cigarettes as a disruptive technology65 that would compete with the established multinational cigarette company brands. By 2014, all the major multinational tobacco companies had entered the e-cigarette market. They did so either by buying existing e-cigarette companies or by developing their own products.66 The most recent offering currently proving very popular in the US is the JUUL manufactured and sold by a private firm that has recently received major investment from the tobacco industry.67
As the major tobacco companies have moved into, and increasingly dominated, the e-cigarette market, they have also appeared to dominate the political and policy-making environment, just as they did shape conventional cigarette policy in the past.68,69
Different countries around the world have reacted in a variety of ways to the introduction of e-cigarettes in their markets, ranging from no regulations to a ban on e-cigarettes.
The European response; the TPD
The Tobacco Products Directive provides a regulatory framework for e-cigarettes throughout the EU.70 The TPD recognises the harm reduction potential of the products, but also acknowledges the existing uncertainties resulting from gaps in knowledge and contradictory scientific views.71,72
The main objective of the TPD is to coordinate the national laws of EU Member States concerning the manufacture, presentation, and sale of tobacco and related products, taking into account the need to guarantee the highest levels of health protection. The TPD does not, however, strive for the full harmonisation of the e-cigarette market, and certain aspects are decided at national level.
The majority of member states prohibit the use of e-cigarettes in public places and have introduced age restrictions on the purchase of e-cigarettes. Of interest is the decision to restrict domestic advertising and sponsorship activities. The notable exception to this is, surprisingly, in the UK.73
The most important differences between member states are the various restrictions on the use of flavours. Some countries have, or are considering, adopting a ban on all but tobacco flavoured e-liquids. This would be in line with the FDA recommendations to ban flavoured e-liquids at grocery stores and gas stations in the US.74
Government versus commerce
Concerns exist over the apparently ambiguous role of the tobacco industry in government-approved cessation schemes which calls into question the ethics of profiting from an addiction and its treatment.75 The tobacco industry’s role has been seen by some as transitioning from the cigarette business into the nicotine business, normalising the industry and nicotine use76,77 while at the same time legitimising the company role as both partner and producer of innovative nicotine products. This has been described as the ‘pharmaceuticalisation’ of the tobacco industry.76 A good example of this was the approval in 2015 for British American Tobacco (BAT) to receive a medical licence for its e-cigarette (e-Voke).78 Furthermore, the availability of e-cigarettes on the NHS has been supported by PHE,79 although this is not the view of the current NICE guidelines.80
The global cigarette market was worth US$888bn in 2018 and projected to reach a value of US$1,124bn by 2024.81 This represents an attractive potential tax revenue stream for governments. Included in this has been a dramatic rise in the popularity of e-cigarettes.82 It is now estimated that there are 35 million e-cigarette users globally (including heat-not-burn tobacco products).83 The e-cigarette industry in isolation is predicted to grow by 22% annually, and be worth $50bn by 2025.84 This is three times more than the global contact lens market in the same time frame.85
Marketing strategy
There are concerns about the enormous resources being used by the tobacco industry to promote e cigarettes by changing the message to one of ‘lifestyle choice’ rather than as a means of cessation.9 One only has to compare vaping marketing with that of nicotine patches and gum.24
Figure 5: Concern in the US is rising
As an example, consider the recent introduction of the JUUL, marketed as the iPhone of e-cigarettes. E-cigarette devices have evolved substantially over recent years,86 from the early-generation cigarette-like e-cigarettes (figure2) to more advanced modifiable tank style e-cigarettes87 (figure 3) and now to the emergence in 2015 of sophisticated, sleekly designed, discreet high-tech devices like JUUL (figure 4).88
The JUUL has two basic components: the device, being a flat, rectangular, portable e-cigarette fashioned to look like a computer USB drive89 which includes a temperature regulation system and a battery that is rechargeable at a USB port.90 The second part is the e-liquid cartridge, or ‘JUULpod,’ which also serves as the mouthpiece.86 JUUL is manufactured to be a closed or non-modifiable system.91
The JUUL’s popularity, having almost 75% of the US e-cigarette market,92 is due in part to its trendy, discreet design and youth-friendly flavours, such as apple, berry, mango and crème brûlée. It uses a proprietary e-liquid formula (JUUL salts), based on nicotine salts rather than free-based nicotine, and one pod equates to the nicotine in a pack of cigarettes.93 Consequently, JUUL is said to create an experience more like combustible cigarette smoking than that found with other e-cigarettes on the market.88,89 This is an attribute that appeals to both young and adult smokers.90
Since the cornerstone of the strategy of the tobacco industry has been to market to the youth,94 it should not be surprising that the e-cigarette uptake of this group in the US has reached alarming levels, with over 20% of high school (secondary school-age) students, some 3.6 million people, currently using e-cigarettes.95 This, coupled with a general acceptance of the gateway effect in the US, has resulted in the US surgeon general recently publishing an advisory document on e-cigarettes (and JUUL specifically) warning of the dangers of vaping, now epidemic among the youth (figure 5).15
Over 70% of e-cigarette business is conducted online,96 with most existing e-cigarette companies operating websites or other web-based selling systems.98 There appears to be a distancing of products away from tobacco98 by e-cigarette manufacturers, by using a variety of techniques such as changing the terminology used to ‘vaping’ as opposed to smoking (figure 6).82 The aesthetic appeal is being promoted, including attractiveness, coolness, colours, and innovative packaging and flavour variations. In addition, there is also evidence of celebrity endorsements and sports sponsorship.99
Figure 6: Example of advertising aimed at younger people
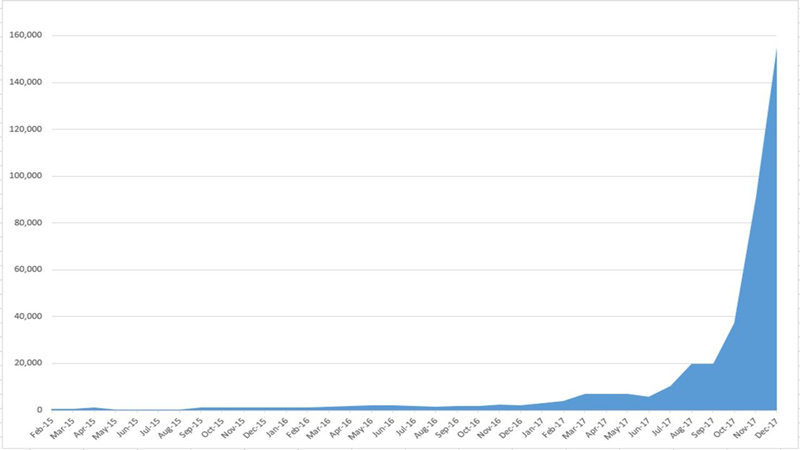
Social media has become a powerful tool for spreading the pro-vaping message by the vaping industry and its advocates (figure 7). Research into the success of JUUL’s have concluded that social media activities were highly correlated retail sales. Targeted cross-platform social media campaigns, with little investment, can have substantial influence on people’s attitudes, beliefs and behaviours related to these products.86 There is little in the way of the public health field reflecting the clinical point of view in ongoing social media dialogues. This highlights the need for public health bodies to interact with the public to actively influence social media conversations and create a more balanced discussion.82
Why should ECPs be aware?
Though the evidence base regarding the ocular impact of e-cigarettes is far from comprehensive, an increasing number of reports suggest a strong association between the use of vaping and direct adverse effect, mainly through ocular surface disease, and indirect impact, particularly through the impact upon cardiovascular health of inhaled chemicals.
Figure 7: Number of JUUL related tweets on Twitter 2015-1786
There is currently little research regarding the ocular impact of e-cigarettes,100 although some professional bodies have produced patient leaflets101 highlighting the public health dangers of smoking and e-cigarettes.
Of the research that is available, the direct ocular impact of e-cigarette’s appears to be at the ocular surface. The vapour contains potentially toxic chemical, such as acrolein and formaldehyde which can cause ocular irritation and dry eye.102-104
Other effects on the eye are more related to the influence of nicotine and include:
- The speeding up of diabetic retinal changes105
- Playing a role in diabetic macular oedema development106
- Reduction in blood flow in microvascular beds and contributing to macular degeneration107
Conclusion
E-cigarettes are one of the most controversial issues in public health today. Although they are less harmful than smoking, there is disagreement on the level of risk reduction, as they are not absolutely harmless. It will take years to generate final conclusions about the clinical effects of switching from tobacco to e-cigarette use. More research is needed into the interactions between smoking and e-cigarette use in adolescents and to examine whether e-cigarettes are a source of harm or harm reduction in this population.9
Given what we know about the ocular impact of conventional smoking upon systemic and ocular health, it is important for all eye care practitioners to keep up to date in this area so as to be better able to offer appropriate advice to both existing smokers, vapers and those who may express a concern or interest. •
Dr Rohit Narayan is a therapeutic optometrist based in the Midlands.
References
- Hartmann-Boyce J, Begh R, Aveyard P. Electronic cigarettes for smoking cessation. BMJ 2018; 360: j5543.
- Ferkol TW, Farber HJ, La Grutta S, et al. Electronic cigarette use in youths: a position statement of the Forum of International Respiratory Societies. Eur Respir J 2018; 51: 1800278
- National Academies of Sciences, Engineering, and Medicine. 2018. Public health consequences of e-cigarettes. Washington, DC: The National Academies Press. doi:https://doi.org/10.17226/24952
- Gaga M, Welte T, Troosters T, Bush A. (2018) Electronic cigarettes for smoking cessation. Br Med J http://www.bmj.com/content/360/bmj.j5543/rapid-responses
- Green S et al. Evidence, Policy, and E-Cigarettes — Will England Reframe the Debate? N Engl J Med 2016; 374:1301-1303
- Ghosh A, Coakley RC, Mascenik T, et al. Chronic E-cigarette Exposure Alters the Human Bronchial Epithelial Proteome. Am Rev Respir Crit Care Med 2018; 198: 67-76
- Benowitz, Neal L. Nicotine addiction. New England Journal of Medicine 362.24 (2010): 2295-2303
- Hsu, Greta, Jessica Y. Sun, and Shu-Hong Zhu. “Evolution of electronic cigarette brands from 2013-2014 to 2016-2017: analysis of brand websites.” Journal of medical Internet research 20.3 (2018): e80
- Bush A, Bhatt J, Grigg J. E cigarettes: Tar Wars: The (Tobacco) Empire Strikes Back. Arch Dis Child 2018 Nov 29; pii: archdischild-2018-315820
- Green, Lawrence W., Jonathan E. Fielding, and Ross C. Brownson. “The debate about electronic cigarettes: harm minimization or the precautionary principle.” Annual review of public health 39 (2018): 189-191
- Alzahrani, Talal, et al. “Association between electronic cigarette use and myocardial infarction.” American journal of preventive medicine 55.4 (2018): 455-461
- Kandel ER, Kandel DB. A molecular basis for nicotine as a gateway drug. N Engl J Med. 2014;371(10):932–943
- Office of the Surgeon General. The Health Consequences of Smoking-50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention (US), National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014. https://www.surgeongeneral.gov/library/reports/50-years-of-progress/full-report.pdf
- Office of the Surgeon General. E-cigarette Use among Youth and Young Adults: A Report of the Surgeon General. Washington, DC: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2016. www.cdc.gov/tobacco/data_statistics/sgr/e-cigarettes/pdfs/2016_sgr_entire_report_508.pdf
- Office of the Surgeon General. Surgeon General’s Advisory on E-cigarette Use Among Youth. Washington, DC: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2018. https://e-cigarettes.surgeongeneral.gov/documents/surgeon-generals-advisory-on-e-cigarette-use-among-youth-2018.pdf
- Tanvir Walelea, Jim Bush, Annelize Koch, Rebecca Savioz, Claire Martin, Grant O’Connell. Evaluation of the safety profile of an electronic vapour product used for two years by smokers in a real-life setting. Regulatory Toxicology and Pharmacology, 92 (2018) 226–238
- Globally Harmonized System of Classification and Labelling of Chemicals – GHS. 4th Rev. New York: United Nations; 2011. http://www.unece.org/fileadmin/DAM/trans/danger/publi/ghs/ghs_rev04/English/ST-SG-AC10-30-Rev4e.pdf”>Rev4e.pdf
- Directive 2015/40/EU of the European Parliament and of the Council of 3 April on the approximation of the laws, regulations and administrative provisions of the Member States concerning the manufacture, presentation and sale of tobacco and related products and repealing Directive 2001/37/EC. Available from http://eur-lex.europa.eu/legal-content/cn/TXT/?uri-CELEX%3A3201410040
- Diver WR, Jacobs EJ, Gapstur SM. Second-hand Smoke Exposure in Childhood and Adulthood in Relation to Adult Mortality Among Never Smokers. Am J Prev Med 2018; 55: 345-52
- Schober W, Szendrei K, Matzen W, et al. Use of electronic cigarettes (e-cigarettes) impairs indoor air quality and increases FeNO levels of e-cigarette consumers. J Hyg Environ Health. 2014; 217: 628–637
- Electronic Nicotine Delivery Systems - section on tobacco control. Pediatrics Nov 2015, 136 (5) 1018-1026; DOI: 10.1542/peds.2015-3222
- Khachatoorian, Careen, et al. “Electronic cigarette chemicals transfer from a vape shop to a nearby business in a multiple-tenant retail building.” Tobacco control (2018)
- Nutt DJ, Phillips LD, Balfour D, et al. Estimating the harms of nicotine-containing products using the MCDA approach. Eur Addict Res 2014; 20: 218-225
- McKee M, Bareham D. E-cigarettes and English exceptionalism. Journal of Health Inequalities. 2018;4(2):68-69. doi:10.5114/jhi.2018.83576
- NICE Guidelines NG92: Stop smoking interventions and services (2018) https://www.nice.org.uk/guidance/ng92/chapter/Rationale-and-impact#advice-on-ecigarettes-2
- European Respiratory Society. We have not learned: ERS leaders respond to BMJ article on the use of e-cigarettes for smoking cessation. Eur Respir Soc 2018. Available from: https://www. ersnet.org/the-society/news/we-have-not-learned:-ers-lead- ers-respond-to-bmj-article-on-the-use-of-e-cigarettes-for- smoking-cessation
- Greenberg, Aryeh, and Ricardo J. Jose. Public Health England prematurely endorses e-cigarettes. BMJ 360 (2018)
- Combes RD, Balls M. A critical assessment of the scientific basis, and implementation, of regulations for the safety assess- ment and marketing of innovative tobacco-related products. Altern Lab Anim 2015; 43: 251-290
- Public Health England - Evidence review of e-cigarettes and heated tobacco products. Available at; https://www.gov.uk/government/publications/e-cigarettes-and-heated- tobacco-products-evidence-review
- National Academies of Sciences, Engineering, and Medicine. 2018. Public health consequences of e-cigarettes. Washington, DC: The National Academies Press. doi:https://doi.org/10.17226/24952
- Chapman, Simon, David Bareham, and Wasim Maziak. The gateway effect of e-cigarettes: reflections on main criticisms. Nicotine & Tobacco Research (2018)
- Bauld L, MacKintosh AM, Eastwood B, et al. Young people’s use of e-cig-arettes across the United Kingdom: findings from five surveys 2015–2017. Int J Environ Res Public Health. 2017;14(9):973
- Health & Social Care Information Centre. Statistics on Smoking, England – 2016. https://digital.nhs.uk/catalogue/PUB20781
- Centers for Disease Control and Prevention (CDC). Electronic Cigarettes (2016). https://www.cdc.gov/tobacco/basic_information/e-cigarettes/index.htm
- Soneji S, Barrington-Trimis JL, Wills TA, et al. Association between initial use of e-cigarettes and subsequent cigarette smoking among adolescents and young adults: a systematic review and meta-analysis. JAMA Pediatrics. 2017;171(8):788–797
- Barrington-Trimis JL, Urman R, Berhane K, et al. E-cigarettes and future cigarette use. Pediatrics. 2016;138(1):1–8.
- Primack BA, Soneji S, Stoolmiller M, Fine MJ, Sargent JD. Progression to traditional cigarette smoking after electronic cigarette use among US adolescents and young adults. JAMA Pediatrics. 2015;169(11):1018–1023
- Dutra L, Glantz S. E-cigarettes and national adolescent cigarette use: 2004–2014. Pediatrics. 2017;139(2)
- Etter J F. Gateway effects and electronic cigarettes. Addiction. 2017 doi:10.1111/add.13924
- Birge M, Duffy S, Miler JA, Hajek P. What proportion of people who try one cigarette become daily smokers? A meta analysis of representative surveys. Nicotine Tobacco Research 2017. doi:10.1093/ntr/ntx243.
- Fidler JA, Wardle J, Brodersen NH, Jarvis MJ, West R. Vulnerability to smoking after trying a single cigarette can lie dormant for three years or more. Tobacco Control. 2006;15(3):205–209
- U.S. Department of Health and Human Services. E-Cigarette Use Among Youth and Young Adults. Altanta, GA: A Report of the Surgeon General, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2016.
- DiFranza JR, Rigotti NA, McNeill AD, et al. Initial symptoms of nicotine dependence in adolescents. Tobacco Control. 2009(3):313–319.
- DiFranza JR, Savageau JA, Rigotti NA, et al. Development of symptoms of tobacco dependence in youths: 30 month follow up data from the DANDY study. Tob Control. 2002;11(3):228–235
- Doubeni CA, Reed G, Difranza JR. Early course of nicotine dependence in adolescent smokers. Pediatrics 2010; 125: 1127–1133
- Blundell, M., P. Dargan, and D. Wood. A cloud on the horizon–a survey into the use of electronic vaping devices for recreational drug and new psychoactive substance (NPS) administration. QJM: An International Journal of Medicine 111.1 (2017): 9-14
- Royal Society for Public Health. www.rsph.org.uk/about-us/news/undercover-investigation-finds-9-in-10-vape-shops-prepared-to-sell-to-non-smokers.html
- Fulton E, Gokal K, Griffiths S, Wild S. More than half of adolescent E-cigarette users had never smoked a cigarette: findings from a study of school children in the UK. Public Health 2018; 161: 33-5#
- Conner M, Grogan S, Simms-Ellis R, Flett K, Sykes-Muskett B, Cowap L, Lawton R, Armitage CJ, Meads D, Torgerson C, West R, Siddiqi K. Do electronic cigarettes increase cigarette smoking in UK adolescents? Evidence from a 12-month prospective study. Tob Control. 2017 Aug 17. pii: tobaccocontrol-2016-053539.
- O’Connell, Grant, et al. A randomised, open-label, cross-over clinical study to evaluate the pharmacokinetic profiles of cigarettes and e-cigarettes with nicotine salt formulations in US adult smokers. Internal and emergency medicine (2019): 1-9.
- McNeill, Ann, et al. Evidence review of e-cigarettes and heated tobacco products 2018. A report commissioned by Public Health England. London: Public Health England 6
- McRobbie, Hayden, et al. Electronic cigarettes for smoking cessation and reduction. Cochrane Database of systematic reviews 12 (2014)
- Schroeder, Megan J., and Allison C. Hoffman. “Electronic cigarettes and nicotine clinical pharmacology.” Tobacco control 23.suppl 2 (2014): ii30-ii35.
- Farsalinos, K. Electronic cigarettes: an aid in smoking cessation, or a new health hazard? Therapeutic advances in respiratory disease 12 (2018): 1753465817744960
- Cipolla, David, and Igor Gonda. Inhaled nicotine replacement therapy. Asian Journal of Pharmaceutical Sciences, 10.6 (2015): 472-480
- Caldwell, Brent, Walt Sumner, and Julian Crane. A systematic review of nicotine by inhalation: is there a role for the inhaled route? Nicotine & Tobacco Research 14.10 (2012): 1127-1139
- McNeill, A., et al. E-cigarettes: an evidence update. Public Health England 3 (2015)
- Royal College of Physicians (2016) Nicotine without smoke: tobacco harm reduction. https://www.rcplondon.ac.uk/projects/outputs/nicotine-without-smoke-tobacco-harm-reduction-0
- Glantz SA, Bareham DW. E-Cigarettes: Use, Effects on Smoking, Risks, and Policy Implications. Annual Rev Public Health 2018; 39: 215-235
- Bullen C, Howe C, Laugesen M. Electronic cigarettes for smoking cessation: a randomised controlled trial. Lancet 2013; 382: 1629-37
- Halpern SD, Harhay MO, Saulsgiver K, Brophy C, Troxel AB, Volpp KG. A Pragmatic Trial of E-Cigarettes, Incentives, and Drugs for Smoking Cessation. N Engl J Med 2018; 378: 2302-2310
- Kalkhoran S, Glantz SA. E-cigarettes and smoking cessation in real-world and clinical settings: a systematic review and meta-analysis. Lancet Respir Med 2016; 4: 116-28
- Apollonio, Dorie, and Stanton A. Glantz. Tobacco industry research on nicotine replacement therapy: If anyone is going to take away our business it should be us. American Journal of Public Health, 107.10 (2017): 1636-1642
- Dunn P. Response to BAT industries’note on transdermal nicotine. 1992. Batesno. 500872836–500872837. Available at: https://industrydocuments.library.ucsf.edu/tobacco/docs/zfbh0045
- Stimson GV, Thom B, Costall P. 2014. Disruptive innovations: the rise of the electronic cigarette. Int. J. Drug Policy 25:653–55
- Tobacco Tactics. 2016. E-cigarettes. Updated July 5, Univ. Bath, Bath, UK. http://www.tobaccotactics.org/index.php/E-cigarettes
- CNBC (2018) https://www.cnbc.com/2018/12/20/altria-takes-stake-in-juul-a-pivotal-moment-for-the-e-cigarette-maker.html
- Cox E, Barry RA, Glantz S. 2016. E-cigarette policymaking by local and state governments: 2009–2014
- Lempert LK, Grana R, Glantz SA. 2016. The importance of product definitions in US e-cigarette laws and regulations. Tobacco Control, 25:e44–51
- Tobacco Products Directive 2014. Official Journal of the European Union. Available at; https://ec.europa.eu/health/sites/health/files/tobacco/docs/dir_201440_en.pdf
- Bates C. What is wrong with the Tobacco Products Direc-tive for vapour products? The Counterfactual, 22 May 2015. Available from: https://www.clivebates.com/what-is-wrong-with- the-tobacco-products-directive-for-vapour-products/
- EUPHA. Facts and fiction on e-cigs. 2018. Available from: https://eupha.org/repository/advocacy/EUPHA_facts_and_ fiction_on_e-cigs.pdf
- Gruszczyński, Łukasz. The EU regime for e-cigarettes: A rational compromise or regulatory failure? Journal of Health Inequalities 4.2 (2018): 62-67
- McGinley L. FDA plans curbs on e-cigarette sales over concerns about surge in teen vaping, The Washington Post, 8 November 2018. Available from: https://wapo.st/2Dfxl58
- World Health Organization. Guidelines for implementation of Article 5.3 of the WHO Framework Convention on Tobacco Control.2008
- Hendlin YH, Elias J, Ling PM. The Pharmaceuticalization of the Tobacco Industry. Ann Intern Med. 2017;167:278–280. doi: 10.7326/M17-0759
- Royal Pharmaceutical Society. E-Cigarettes Policy Recommendations, 2014. Available at; https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Policy%20statements/E-Cigarettes%20Policy%20Statement.pdf
- Medicines and Healthcare Products Regulatory Agency, 2015. Available at; http://www.mhra.gov.uk/home/groups/par/documents/websiteresources/con616843.pdf
- Public Health England. Evidence review of e-cigarettes and heated tobacco products 2018. A report commissioned by Public Health England. Available at; https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/684963/Evidence_review_of_e-igarettes_and_heated_tobacco_products_2018.pdf
- NICE guideline [NG92], Stop smoking interventions and services, 2018. Available at; www.nice.org.uk/guidance/ng92
- Research & Markets (2019): Cigarette Market: Global Industry Trends, Share, Size, Growth, Opportunity and Forecast 2019-2024. Available at; www.researchandmarkets.com/research/qj2jd5/global_cigarette?w=5
- McCausland, Kahlia, et al. The Messages Presented in Electronic Cigarette–Related Social Media Promotions and Discussion: Scoping Review. Journal of Medical Internet Research, 21.2 (2019): e11953
- Tobacco in Australia. Melbourne, Australia: Cancer Council Victoria; 2017. The e-cigarette market. Available at; www.tobaccoinaustralia.org.au/chapter-18-harm-reduction/18b-1-the-ecigarettemarket
- BIS Research. Electronic cigarette & e vapor (vaporizer) market research reports. Fremont, California: BIS Research; 2016. Available at; https://bisresearch.com/industry-report/electronic-cigarette-market-size-forecast.html
- Grand View Research. Contact Lens Market Size worth $17.72 Bn by 2025. Available at; www.grandviewresearch.com/press-release/global-contact-lenses-market
- Huang J, Duan Z, Kwok J, et al. Vaping versus JUULing: how the extraordinary growth and marketing of JUUL transformed the US retail e-cigarette market. Tobacco Control 2019;28:146-151
- Barrington-Trimis JL, Gibson LA, Halpern-Felsher B, et al. Type of E-Cigarette device used among adolescents and young adults: findings from a pooled analysis of eight studies of 2166 vapers. Nicotine Tobacco Research, 2018;20:271–4
- Lawler R. Vaporization startup Pax Labs introduces Juul, its next-gen e-cigarette. Techcrunch.com 2015. https://techcrunch.com/2015/04/21/pax-juul/
- Goniewicz ML, Boykan R, Messina CR, Eliscu A, Tolentino J. High exposure to nicotine among adolescents who use Juul and other vape pod systems (‘pods’). Tobacco Control. 2018 Sep 7
- Kee C. Everything you need to know about the JUUL, including the health effects: Buzzfeed News, 2018
- Bellafante G. Cool-looking and sweet, JUUL is a vice teens can’t resist. New York Times, 2018
- www.journalnow.com/business/juul-ends-with-percent-market-share/article_6f50f427-19ec-50be-8b0c-d3df18d08759.html
- Willett JG, Bennett M, Hair EC, et al. Recognition, use and perceptions of JUUL among youth and young adults. Tobacco Control. 2018.Epub ahead of print. doi: 10.1136/tobaccocontrol-2018-054273
- Cummings KM, Morley CP, Horan JK, et al. Marketing to America’s youth: evidence from corporate documents. Tobacco Control 2002;11:i5-i17
- Cullen KA, Ambrose BK, Gentzke AS, Apelberg BJ, Jamal A, King BA. Notes from the field: Increase in use of electronic cigarettes and any tobacco product among middle and high school students in the United States, 2011-2018. Morbidity & Mortality Weekly Report 2018; 67(45):1276-1277
- IFF Research. United Kingdom: HM Revenue and Customs; 2016. Understanding the online e-cigarette market. Available at; https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/565928/Understanding_Online_Ecigarette_market_HMRC-research.pdf
- Zhu S, Sun JY, Bonnevie E, Cummins SE, Gamst A, Yin L, Lee M. Four hundred and sixty brands of e-cigarettes and counting: implications for product regulation. Tobacco Control. 2014;23(Supplement 3):iii3–9
- De Andrade M, Hastings G, Angus K, Dixon D, Purves R. The marketing of electronic cigarettes in the UK. Cancer Research UK. 2013. Available at; www.cancerresearchuk.org/sites/default/files/cruk_marketing_of_electronic_cigs_nov_2013.pdf
- Cancer Research UK, 2014. The marketing of electronic cigarettes in the UK. Available at; www.cancerresearchuk.org/sites/default/files/cruk_marketing_of_electronic_cigs_nov_2013.pdf
- RNIB, 2016. www.rnib.org.uk/nb-online/smoking-increase-risk-amd
- American Optometric Association, 2016. www.aoa.org/Documents/Smoking_Vaping_and_Your_Eyes_FactSheet.pdf
- Mastrota, Katherine M. How vaping affects the ocular surface. Optometry Times, 2017. Available at; www.optometrytimes.com/authors/katherine-m-mastrota-ms-od-faao-dipl-abo
- Davis CP. Vaping (e-Cigarettes) Side Effects, Health Risks, and Safety. Medicinenet 2018, available at; www.medicinenet.com/e-cigarettes_vs_cigarettes/article.htm
- American Cancer Society, 2018. What do we know about E-cigarettes? Available at; www.cancer.org/cancer/cancer-causes/tobacco-and-cancer/e-cigarettes.html
- Boretsky, Adam, et al. Nicotine accelerates diabetes-induced retinal changes. Current Eye Research, 40.4 (2015): 368-377
- Maugeri, Grazia, et al. Role of nicotine during diabetic macular edema development. Italian Journal of Anatomy and Embryology, 122.1 (2017): 141
- Benowitz, Neal L., and Andrea D. Burbank. Cardiovascular toxicity of nicotine: implications for electronic cigarette use. Trends in Cardiovascular Medicine 26.6, (2016): 515-523