In the latest in our CET series on binocular vision, Dr Fergal Ennis took a close look at the cover test. When assessing a patient’s binocular status, the cover test (CT) is one of the first that would be considered by most practitioners. Its advantages are that is relatively quick, non-invasive and easy to perform, with minimal extra equipment required. However, the technique can give misleading results or lead to the omission of important findings. Co-operation by the patient is also required, which can be especially challenging with young children, babies or patients with learning difficulties or communication issues.
The cover test is usually performed at distance and near, and typically after history and symptoms and acuities, with the patient’s habitual spectacle prescription in place where worn. It may then be compared to the test unaided or with a changed prescription if required. It may also be performed at any other significant working distance adopted by the patient in their occupation or hobby, for example an intermediate computer viewing distance, or a very close distance adopted for fine jewellery making.
Technique
The basic techniques for the cover test are summarised in tables 1 and 2 for tests undertaken with patient gaze in the primary position (LE for left eye, RE for right eye from now on).
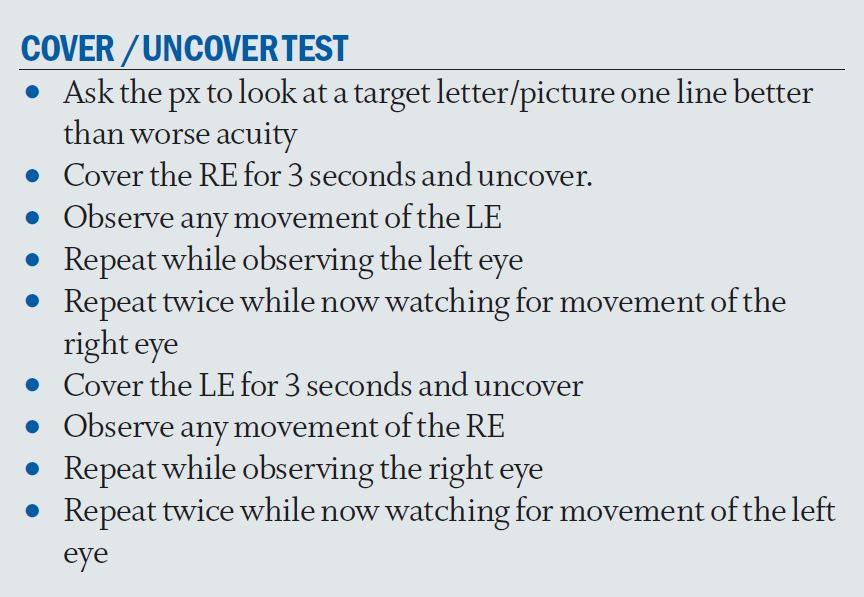
Table 1
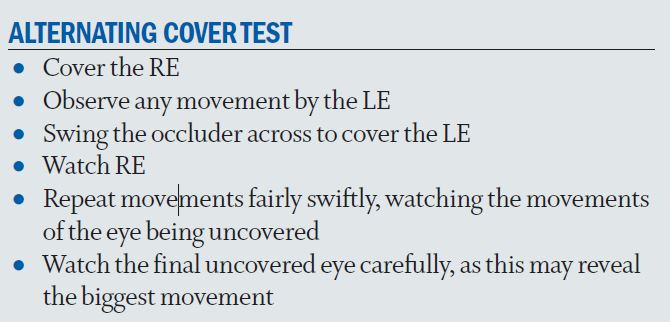
Table 2
Clear instructions need to be given to the patient that while each eye is covered and uncovered, it is important for them to keep looking at the selected target. When moving the occluder, this should be done in a smooth fashion. Position yourself from the patient such that you can view both eyes, even when occluding each eye. Some practitioners advocate the use of a translucent occluder to see any movement behind the cover without risking loss of dissociation by ‘peeking’ (figure 1).

Figure 1: Use of a translucent occluder
The occluder should be held close enough in front of the eye to provide dissociation from the surroundings (about 2cm), but not so close that the px wants to move away from it. Repeat the procedure up to three times to gain adequate results. Too many repeat covers may result in loss of fixation and concentration.
The Cover/Uncover Test
The cover/uncover test is used to detect heterotropia (strabismus) and heterophoria. Concomitant heterotropia and heterophoria will be described here, ie the angle of deviation does not change in different directions of gaze. The theory behind this test is that if both eyes are aligned, they will fixate simultaneously on a target. If either eye is covered, no movement will take place (orthophoria). In a heterotropia (strabismus/ manifest deviation) where one eye may be deviated, when the fixing eye is covered the other eye will move to take up fixation. Its movement will therefore be in the opposite direction of the deviation. For example, a nasal movement will be made for a temporally deviated eye (exotropia), a temporal movement in a nasal deviation (esotropia), a downward movement will be seen for a superiorly deviated eye (hypertropia) and an upward movement in an inferior deviation (hypotropia). There can be mixed components, so a diagonal movement would be seen in a combination of the above example. For ease, it may be simpler to always try to note the horizontal components and then figure the vertical components separately.
As the cover is removed, two things could happen. If the deviation is on one eye only, for example where there is a left exotropia, the LE will deviate out again and the RE will move nasally to retake up fixation. In other words, both eyes will move in the same direction on removing the cover. This would also apply to the vertical deviations, both eyes would appear to move up together (in a hypotropia) or down together (in a hypertropia). These are called recovery movements. The second thing that could occur is that there is an alternating deviation, in which case the uncovered eye would not move. In this example, the RE would then move only on occlusion of the LE. The rate of recovery should also be noted as this gives an indication of how well compensated the deviation is. A fast movement of the uncovered and covered eye would indicate that good compensation was present. A slow or jerky recovery is present when the eyes have to make an effort to realign.
Once experienced, one can observe both the covered up and uncovered eye together using a semi-opaque occluder or the angling of an opaque occluder technique described above. So, for example, covering the RE in a L esotropia would reveal the RE moving to the left nasally and the LE moving to the left temporally. Vertical deviations are usually harder to spot as often they are smaller in magnitude. Look for movement of the position of lid margins.
Exercise
There are four cases for you to consider online:
- A large movement in one eye
- Potential poorly performed test
- An atypical distance cover test
- Atypical near cover test results
Careful consideration of what you see should help to understand what, in at least two of the videos, might at first not seem to make sense. I hope you enjoy the challenge.