Earlier this year, we ran an interactive exercise looking at attitudes to eye care professionals raising the subject if smoking with patients. The general consensus from participants was that, as smoking represented a significant modifiable risk factor for eye health, it was perfectly reasonable to ask about smoking and be prepared to offer appropriate advice if, once in full possession of the facts about is health implications, a patient showed interest in getting some help.1
It may not have escaped readers notice that recent health campaigns have raised the issue of obesity as a risk factor. Indeed, one controversial campaign by Cancer Research UK has even used a simulated cigarette packet to emphasise the significance of obesity as a contributory factor for developing cancer (figure 1). The campaign gained a high profile, but also attracted criticism of ‘fat shaming’ from some quarters.
Figure 1: Cancer Research UK campaign posters established obesity as a risk factor to be considered alongside smoking
Obesity Prevalence
This month, NHS Digital published the latest figures for obesity prevalence.2 The report presented findings from the Government’s National Child Measurement Programme (NCMP) for England for the 2018 to 2019 school year. It looked at children in reception class (aged four to five years) and year six (aged 10 to 11 years) in mainstream state-maintained schools in England and analysed their body mass index (BMI) classification rates by age, sex and ethnicity as well as geographic analyses. BMI divides the weight in kilograms by the square of the person’s height in metres. Table 1 shows generally used BMI assessments.
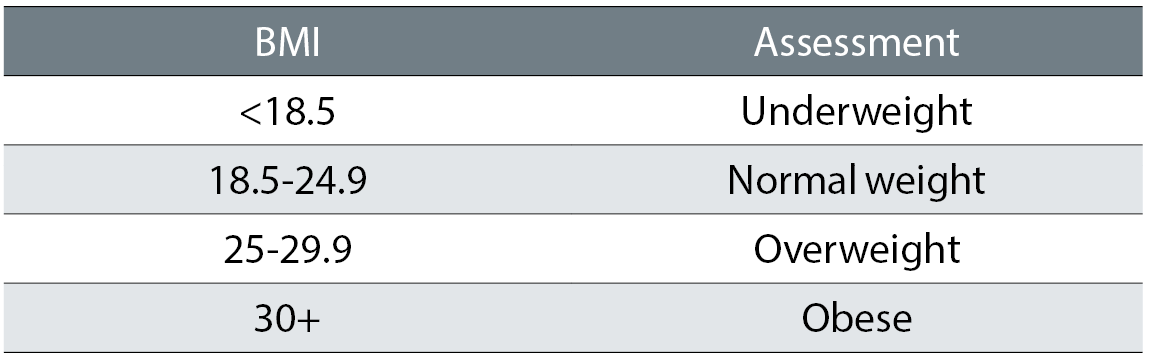
Table 1: Interpreting body mass index
Among the many stark figures were the following:
- In reception, obesity prevalence was 9.7%
- In year six obesity prevalence was 20.2%
- Obesity was higher in boys in reception (10%), and 22.5% of year six boys were obese
- Obesity prevalence for children living in the most deprived areas was more than double that of those living in the least deprived areas for both age groups, and this division is increasing (figure 2)
- Children’s overweight and obesity was associated with that of their parents
- The majority of adults in England in 2017 were overweight or obese (64%)
- Morbid obesity has also increased, from fewer than 1% in 1993, to nearly 4% in 2017
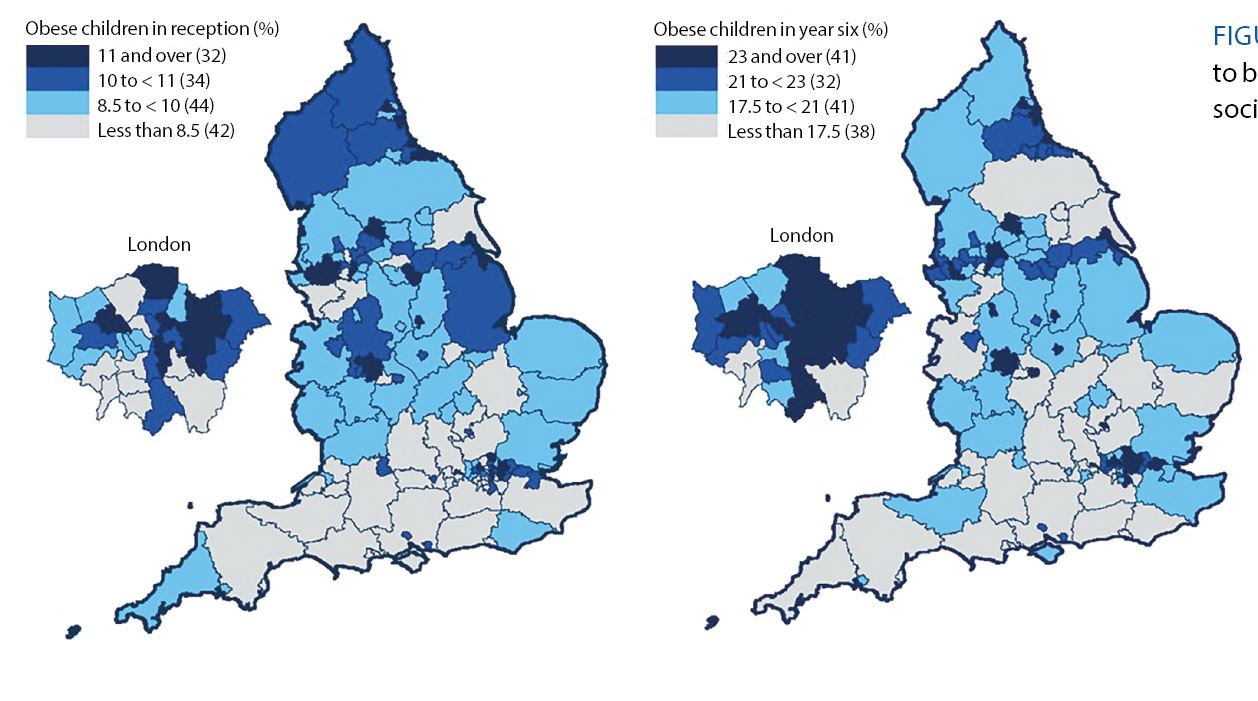
Figure 2: Obesity seems to be related to socioeconomic area 2
Eye Care
Over the past few years, Optician has published CET articles discussing the link between obesity and eye health. Links to these can be found online and are to be referred to before completing the interactive exercise.
As demonstrated by the figures already described, obesity is an escalating concern and a major risk factor for several chronic systemic diseases. Those known to have a strong association with obesity include:3
- Hypercholesterolaemia
- High blood pressure
- Cardiovascular diseases (CVD) – such as arteriosclerosis, atherosclerosis occlusive disorders and disorders of the heart
- Stroke (cerebrovascular accident or CVA)
- Obstructive sleep apnoea (OSA)
- Malignant disease – a number of malignant disorders have association with obesity
- Osteoarthritis
- Diabetes mellitus (DM) – the increase in incidence of type 2 diabetes has reflected obesity increases
Changes in the recent socioeconomic environment, lifestyle, and food consumption, as well as an increase in urbanisation have contributed to this rise.
As with so many lifestyle influences upon health, it is extremely difficult to establish the exact risks associated with obesity. As explained in an excellent review of obesity impact upon eye health, Cheung and Wong explain: ‘Associations of obesity with cataract, glaucoma, age-related maculopathy and retinopathy have been reported with varying degrees of certainty. The inconsistency of results, combined with the deficiency of robust data, suggest that further investigations are required to clarify these associations. The efficacy of obesity treatment in reducing the risk of eye diseases is also unknown.’4 The paucity of good data is most likely due to the difficulties in controlling for the very many other influences upon our eyes over long time periods.
ECP Intervention
So, is it the role of an eye care professional to address obesity if presented with a patient clearly meeting this description? The College of Optometrists has produced a leaflet for patients called Lifestyle and eyes.5 Among various risk factors for eye health that are part of everyday life, there is a short section on obesity which read as follows: ‘Maintaining a healthy weight is not only good for your general health, but it is also good for your eyes. People who are overweight are more likely to develop diabetes, which in turn may affect your eyes. They are also more at risk of developing late AMD and cataracts. Maintaining a healthy weight is also more likely to help you to keep your blood pressure under control. Having high blood pressure can also affect your eyes.’
The leaflet concludes with the following suggestion to patients; ‘For more information, please talk to your local optometrist.’ So, what if a patient follows this advice? Or what if you identify a patient who you feel might benefit from this advice but has not sought it for themselves? It is this that forms the basis of this month’s interactive exercise.
Interactive Exercise
The interactive exercise is related to the management of a patient who appears to be clinically obese. This exercise is designed to encourage discussion about giving information about the links between obesity and ocular health, and further, whether this might be offered without the patient’s initial request. On this latter point, there may be a divergence of views. This is to be expected and now is the time to encourage a healthy debate on this topic.
Before you attempt the exercise, there are six multiple choice questions which assess an overall understanding of obesity. To ensure successful completion, the relevant source material is available here:
Remember:
- There is no one single answer for your discussion, but what is needed is a reflection of your discussion (which must be for a minimum of 10 minutes please) that is sufficient evidence of the various points having been covered.
- Read the source material available.
- Complete six multiple choice questions to confirm you have grasped the main concepts.
- Read the case scenario about which you are to confer with a registered colleague.
- The exercise is designed for both optometrists and dispensing opticians, so please ensure your discussion is relevant to your own role and responsibility.
- Confirm with us the name and GOC registration number of the colleague with whom you have discussed the case and also write some short notes on the outcome of your discussion.
- At the end of the month’s active period we will confirm that your discussion outcome meets the requirement for an interactive point.
- Look out for a published discussion based on all responses in a future issue of Optician.
References
- Harvey B. Smoking interactive. Optician, 09.08.2019, pp 32-35
- NHS Digital. Statistics on Obesity, Physical Activity and Diet, England, 2019. Available at; https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-obesity-physical-activity-and-diet/statistics-on-obesity-physical-activity-and-diet-england-2019/part-3-adult-obesity
- Gherghel D, Ramchandani N. Obesity and ocular health. Optician, 19.04.2019, pp 26-31
- Cheung, N and TY Wong. Obesity and Eye Diseases. Survey of Ophthalmology, 2007; 52(2): p 180-195
- Lifestyle and eye leaflet. Downloadable from; www.college-optometrists.org/membership/free-patient-resources/patient-leaflets.html