I have often stated that the world is full of hand magnifiers gathering dust in drawers. I remember when I started in low vision, a successful outcome was to have given out a magnifier that achieved the calculated predicted target acuity. Thankfully, I soon learned from my patients that a more useful approach was to listen to them, find out what they wanted to know about the cause of their sight loss, find out how they felt about their loss, build up a picture of their world and, finally, to offer appropriate support and advice, either from me or someone better suited, on an ongoing basis. Sometimes this involves giving a magnifier.
I also remember how magnification through systems other than single lens systems were described as ‘complex’. And where the image was displayed upon on a screen, the system was described as a CCTV. At that time, as many of the latter were basically a lens system, converter and cathode ray tube television screen, and because the signal between the input and output was not broadcast beyond the unit, then the term ‘closed circuit television’ just about applied. Why the term CCTV is still being used to refer to all sorts of electronic magnification devices (see the latest pre-reg assessment framework, for example) is beyond me.
Even in the old days of CCTVs, there were clear advantages with electronic displays in the way that field of view could be maximised and the image itself could be enhanced, manipulated or framed in ways to optimise for individual viewing. The great advances in digital information over recent years have resulted in many benefits for those with sight loss, and CCTVs have been superseded by devices that allow a whole range of image adaptations. It is these that this series will focus upon. In future articles, we will focus on equipment specifically designed for the visually impaired and describe some of the impressive functionality now available. Before that, I would first like to offer some points about what might be achieved using technology that, far from deserving the label ‘complex’, is likely to be found in the home, pocket or bag of most people these days.
Demographic Evolution
I recently heard an amusing discussion about how technology usage can help identify someone’s age with worrying accuracy. Email, YouTube, Facebook, Twitter, WhatsApp, SnapChat, TikTok; name your usage, give away your age. I am a fan of vinyl and VHS, but even I know that you tend to prefer what you understand or are familiar with. For too many years, it was wrongly assumed that the elderly, and therefore in most cases those seeking help with sight loss, were ‘computer illiterate’ except for a few ‘silver surfers’. While at one time there was, perhaps, some truth in this, it is absolutely a mistake to relate ability to age, especially with regard to a non-physical activity such as use of electronic equipment. Elderly people meet younger people, use broadcast media and show interest in any new development that might be of benefit. Add to that any major societal change, such as has happened since last March, and familiarity with the previously obscure is accelerated.
So, may I just emphasise an important point; people over 60 are familiar with and use electronic equipment.
A quick glance at the Office for National Statistics website (www.ons.gov.uk) appears to support the stereotype. Figure 1, for example, shows that use of the internet is universal among younger age groups, but less than half of the over 65s use it. But if you look more closely into the figures, some interesting facts arise. For example, between 2011 and 2019, the age group found to have the largest increase in recent internet use is the 65 to 74-year-olds (figure 2).
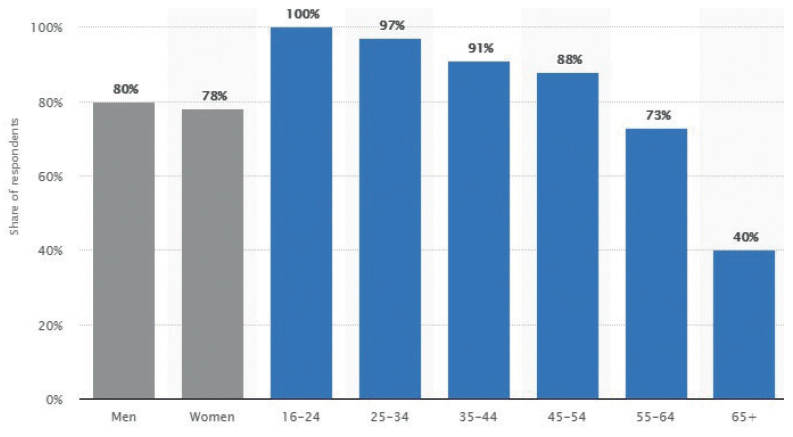 Figure 1: Access to the internet by age (source; ONS UK)
Figure 1: Access to the internet by age (source; ONS UK)
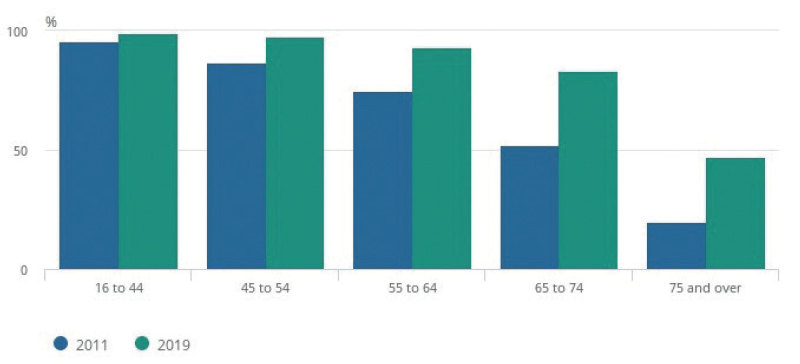 Figure 2: Recent internet users by age in 2011 and 2019 (source; ONS UK)
Figure 2: Recent internet users by age in 2011 and 2019 (source; ONS UK)
What really brought this home to me was when, some five years ago now, I spent a good deal of time demonstrating a low power hand magnifier to an elderly patient. During the consultation, her phone beeped its receipt of a text message. She promptly took out her phone and read the message, explaining ‘my nephew has made the print easy for me to read. I wish he could do this for the newspaper.’ As it turned out, font size change was just one of a whole host of things she could have enjoyed. And since then, she has learned to use her phone as an illuminated hand magnifier. I assume my simple aid has long since joined the dust gatherers.
A Note on Terminology
The term CCTV is best left to security systems. A more appropriate general term for the electronic display of an image that may allow for enhancement might be electronic magnification. Indeed, in recent years, many authorities have adopted the term electronic vision enhancement systems, often simply stated as EVES, to describe kit that allows this. But even this term is somewhat constraining. Take, for example, the increasingly familiar OrCam system (figure 3), a spectacle worn device which converts an image to an audible descriptive signal. Or what about a text reading app on a smartphone. Whether either fit the EVES definition might be debated.
 Figure 3: The OrCam; a visual input is converted into an audio signal
Figure 3: The OrCam; a visual input is converted into an audio signal
So there has been a move towards more general terminology to describe any technology that may help an individual with an impairment. The terms it is definitely worth being familiar with are as follows:
- Assistive technology; this is the blanket term for anything that might be used by someone with an impairment to assist them, even though this was not the primary function of the technology. As a simple illustration of this, consider a walking stick. This could be used by anyone, but a person with a mobility impairment might find it extremely useful. By the World Health Organisation definition, the term assistive technology refers not just to the product, but also the supply and support services of the product too.1 Assistive technology offers people with disability an opportunity for greater social participation, security and control, and a greater chance to reduce institutional costs without significantly increasing household expenses.2
- Adaptive technology; this is used to refer to a technology whose design is aimed at an end user with an impairment. As such, it is considered a subset of assistive technology. For example, a hearing aid is classed as assistive technology but, as it is aimed at those with a hearing impairment, is also and
perhaps better defined as adaptive technology. To push the definition further, I assume that prescription spectacles count as adaptive technology.
Globally, more than one billion people benefit from one or more assistive products. With an ageing global population and a rise in noncommunicable diseases, more than two billion people will need at least one assistive product by 2030, with many older people needing two or more.1
As we shall discover, there is still some blurring between the terms. For example, consider the patient previously mentioned. Her smartphone might be considered as assistive technology because, though designed for general use, it can be used by someone with a visual impairment in a way that improves their functioning. That said, the specific software incorporated to enhance text might be considered to be adaptive technology as it is designed for and most likely to be used specifically by someone with a visual impairment.
Before you accuse me of semantic noodling, now consider the following point. A person in employment who loses their sight might be able to continue in employment with the help of the Access to Work scheme. This might include help towards the cost of an assistive technology device offering electronic vision enhancement. A new iPad tablet can be adapted to offer the visual enhancement required. However, as it is not classed as a medical device (as defined by the UK Medical Devices Regulations 2002 (Amendment EU Exit) Regulations 20202), then it is not supported by the Action to Work scheme. However, a dedicated adaptive technology system, such as an EVES product, is listed as a medical device and is supported. This is the case even if the iPad is argued to have better functionality or is more economical than a specified adaptive technology medical device.
Achieving clarity as to whether a technology might be designated as a medical device is tricky. The UK competent authority charged with classification of medical devices is the MHRA and has published a guidance to clarify how these products should be classified. They state that any technology will likely be classified as a medical device if there is a direct link between the corrective function of the equipment and the individual concerned.3
But the MHRA also cite examples of how the classification is not straightforward. ‘Cushions which are intended to relieve pressure and prevent pressure sores for use by wheelchair users who spend long hours sitting in the chair would likely be considered to be medical devices because they have a clear medical purpose and a clear link between the corrective function (to relieve pressure and prevent pressure sores) and the individual (wheelchair user). However, ordinary cushions (including those used in hospital or healthcare environments) would not be considered medical devices because their primary purpose is for comfort rather than medical and they can be used by anyone.’
Ultimately, the decision seems to hinge upon a statement from a manufacturer defining who the end user is and confirming that their technology or device is intended to be used by specific individuals for a stated medical purpose. Without this, it is unlikely that the product will be classified as a medical device. Therefore, the classification depends on the claims made by the manufacturer for each product.
So, as technology develops apace, it may well be the case that an eye care professional recommends and advises upon a technology that is not listed as a medical device but, in their view, has both functional and economic benefits for the user.
Everyday Assistive Technology
I will now offer an overview of some commonplace devices and how they are adapted to benefit those with visual impairment. This is by no means a comprehensive guide and, for those wanting more detail, I suggest you jump straight to the useful resource list at the end. I will suggest, however, that everything now mentioned is essential knowledge for anyone who regularly sees people with reduced vision, and not just within a low vision clinic setting.
Television
Most mainstream televisions available today have accessibility features and tools built into them which help to make these devices accessible for people who are blind or partially sighted. I bet readers have accidentally started the audio description setting and wandered who was talking.
Panasonic, Samsung and some other manufacturers include a built-in voice guidance feature in their latest digital televisions which will say out loud on-screen information such as what
channel is on, read out television guides, menus, upcoming and recorded programs, and talk the viewer through changes to settings.
There is much more to be advised these days than ‘sit closer’. I also suggest that such enhancements are worth sorting out before prescribing low vision aids such as a TV Max.
‘Computers’
The inverted commas are there because, by this, I mean laptops and desktops. Many people benefit from some simple adaptations, and many increasingly rely on things like email and online websites to stay in touch with what is happening. Few, I suggest, know how to use accessibility options.
To simplify, there are two main operating software platforms; Microsoft Windows and Apple Mac OS operating systems. Each offers a number of options for viewing enhancement. Both also include a virtual assistant (Cortana and Siri, respectively) that allow voice commands to access various functions on screen.
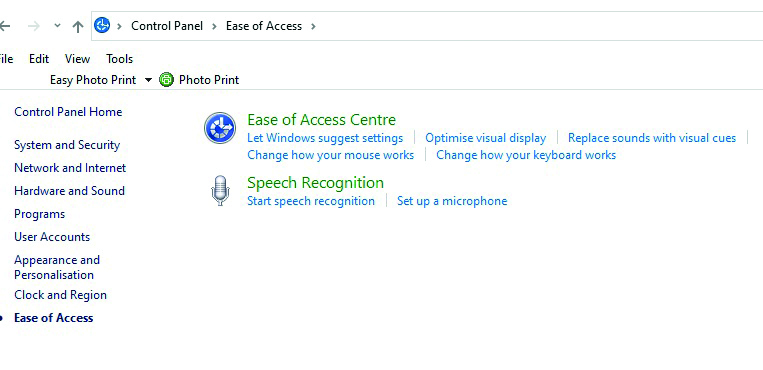
For Windows, the area to go to is the Ease of Access Centre (or Accessibility options on older systems) which I get to by searching for the control panel in the search field (figure 4). For Macs, go to the Finder, choose All Applications and then Accessibility. Next time you have any spare time, make a cup of tea and do this on your own computer. This is the best way to see the many options available (magnification, text enhancements, text to speech and so on) and to also be more confident when offering advice to a patient.
One limitation of these platform settings was that, though useful for in-built programs such as Word or Outlook email, they had no effect on websites being viewed online. Recently, commonly used web browsers have greatly increased their functionality to allow a wide range of enhancements for web-browsing.
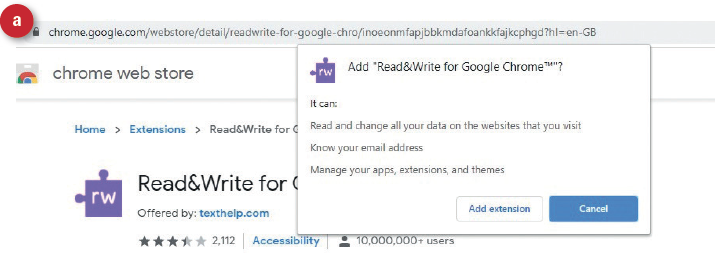
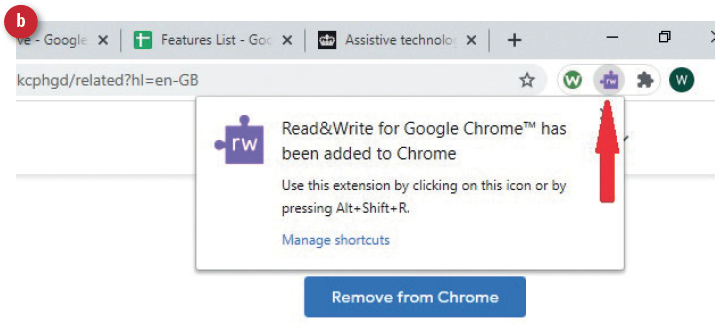
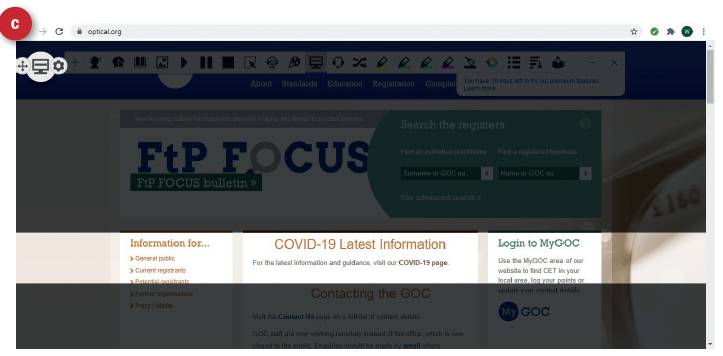 Figure 5: Using Chrome Read&Write
Figure 5: Using Chrome Read&Write
I use Chrome (other browsers are available). When I googled ‘Chrome accessibility’, I was directed to the online Chrome Web Store where I downloaded (for free) the Read & Write add-on (figure 5a). This then placed a small icon in my browser (figure 5b). I then viewed the GOC website and, by clicking the icon, was able to select a whole range of image enhancements, including an adjustable typoscope (5c). I also downloaded the Screenshot reader with a second icon (figure 6a). I could then outline the text I was interest in, press ‘play’ and a perfectly clear voice read out the outlined text. Each word shows blue as it is read, reminding me of the moving dot on the old ‘beer at home’ adverts on TV.
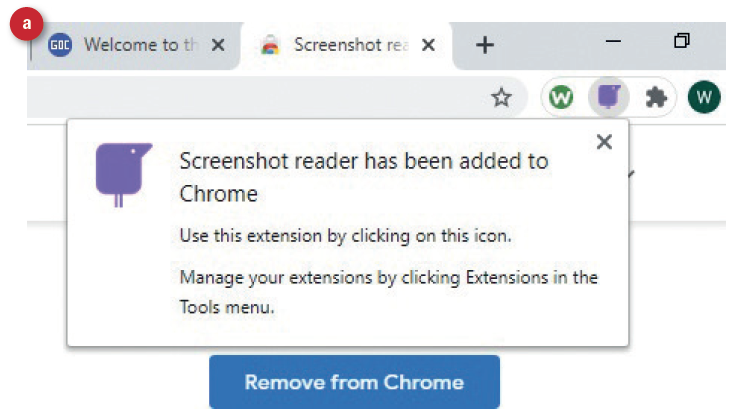
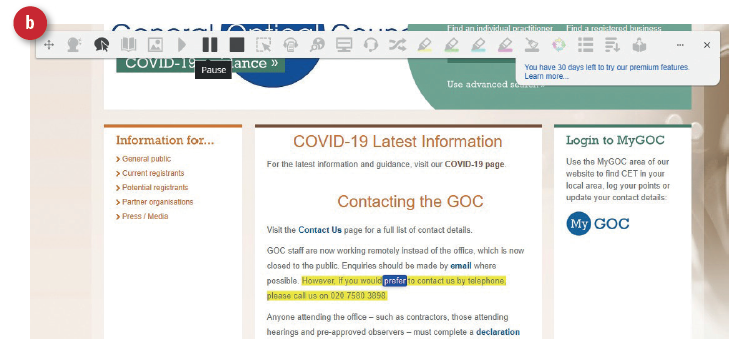 Figure 6: Using Chrome Screenshot reader
Figure 6: Using Chrome Screenshot reader
Bill Harvey is a specialist optometrist at the RNIB.
- Next, this series will focus upon smartphones and tablets.
- The author would like to thank RNIB technology expert Paresh Jotangia for his advice.
References
- World Health Organisation. www.who.int/news-room/fact-sheets/detail/assistive-technology (Accessed February 2021)
- Parant A, Schiano-Lomoriello S, Marchan F. How would I live with a disability? Expectations of bio-psychosocial consequences and assistive technology use. Disability and Rehabilitation: Assistive Technology. 2017, 12 (7): 681–685
- Guidance; Assistive technology: definition and safe use. Updated 12 February 2021 and available at; www.gov.uk/
government/publications/assistive-technology-definition-and-safe-use/assistive-technology-definition-and-safe-use - www.rnib.org.uk/sight-loss-advice/technology-and-useful-products/technology-resource-hub-latest-facts-tips-and-guides/accessible-televisions
Resources
An essential resource is the RNIB Technology resource hub which can be reached at www.rnib.org.uk/practical-help/technology/resource-hub. This includes clear information
and extra resources on:
- TV adaptations, audio description, large print TV guides, etc
- Phones, tablets and desktop adaptation
- Specialist access technology – Braille display, screen readers, screen magnification, smart glasses and head-mounted cameras
- Home assistance – speaker driven assistance for access to media and electrical appliance control
Another essential resource is called My Computer My Way; an essential guide to the many ways you can adjust your laptop, desktop, tablet or smartphone, including changes to your keyboard and mouse. Access this at https://mcmw.abilitynet.org.uk/impairment/rnib-vision.
Another excellent resource is from the US and offers information about computer adaptations. This can be accessed at www.afb.org/blindness-and-low-vision/using-technology/using-computer.
If you are already computer savvy and would like to share your knowledge with those less able, why not consider volunteering as a tech advisor? Go to www.rnib.org.uk/volunteering/search-by-volunteer-category/become-tech-volunteer.
Finally, wherever you are in the UK, if you have a patient who might benefit from skilled advice on computer set up, they can contact the RNIB helpline (0303 123 9999) and ask for the technology team.