Task specific and occupation dispensing is a GOC core competency area for both optometrists and dispensing opticians who should be able to ‘advise on, order and dispense the most suitable form of optical correction taking into account durability, comfort, cosmetic appearance, age and lifestyle.’
Related GOC core competency (4.2.1 for dispensing opticians and 4.1.4 for optometrists) goes on to add: ‘Advises on personal eye protection regulations and relevant standards, and appropriately advises patients on their occupational visual requirements.’
The competencies require registrants to have an understanding of the law, regulations and standards relating to vocational dispensing and apply them in the workplace. This includes rules relating to display screen equipment, driving and eyewear that is protective against physical injury and harmful radiation, which itself includes understanding and being able to identify common ocular hazards and common or sight threatening leisure activities and occupations and advise patients thereon.
Optometrists and dispensing opticians should also ‘demonstrate a knowledge of visual task analysis including lighting’ as well as understanding the legal responsibilities incumbent upon employees, employers, dispensing opticians and optometrists.
All practitioners are expected to be able to understand the need to supply the correct optical appliance for a specific task, and be able to analyse aspects of the visual task, associated working distances and physical and environmental aspects of the workplace which may affect vision, including the impact of the refractive error on the visual task requirement, the importance of illuminance and luminance (covered in the last article in this series, Optician 26.02.2021), and problems associated with glare and its impact on the visual task at hand.
Since there are hundreds of occupations, this includes the ability to advise on and dispense appropriate safety, vocational and special optical appliances. This must be achieved, not by remembering the requirements for each and every job, but by:
- Asking pertinent questions
- Knowing where to find appropriate information regarding both occupational requirements and product availability
- Applying critical thinking skills to solve the individual problem that is presented.
Indoor Tasks
Many job roles are carried out completely indoors and centre around tasks that mainly concern near and intermediate working distances. This will later be discussed in some detail, but it is worth detailing some other considerations first. For example, distance vision may also be important and, in many jobs, communication is also an important aspect that needs to be considered. In any role where a worker is client-facing, from salespeople to doctors and other healthcare professionals, eye contact is an important element in establishing trust and for communicating effectively.
Tasks requiring eye contact, such as when presenting or teaching (figure 1), can be enhanced by the use of an anti-reflection coating, ideally with a residual hue that is itself not distracting. This might be a green or achromatic reflex rather than blue or purple. Many presenters have last minute nerves and, if they smoke, are apt to obtain a last-minute dose of nicotine outside. Photochromic lenses rather give away this habit, but more importantly look temporarily like sunglasses on stage, and are probably best avoided. Patients who are not used to wearing spectacles, but not prepared to try contact lenses, may prefer rimless spectacles for a more natural look (figure 2).
 Figure 1: Presenting requires good eye contact
Figure 1: Presenting requires good eye contact
 Figure 2: Rimless spectacles can provide a more natural look
Figure 2: Rimless spectacles can provide a more natural look
when presenting and public speaking
Indoor tasks and job roles may also present issues that may not always be considered. Chefs, bakers and home cooks may routinely have issues with spectacles steaming up, when for example opening oven doors. This can be a dangerous situation in a busy commercial kitchen (figure 3). Most eye care practitioners have become more familiar during the Covid pandemic with successful anti-fog spectacle lenses and cleaners that they can recommend to this group of patients as an alternative to contact lenses.
 Figure 3: Removing dishes from the oven can result in glasses steaming up; note the condensation when the glass of iced water is held near the hot food. There is a variety of solutions available for the problem when it affects spectacles
Figure 3: Removing dishes from the oven can result in glasses steaming up; note the condensation when the glass of iced water is held near the hot food. There is a variety of solutions available for the problem when it affects spectacles
Many job roles or tasks require accurate colour definition. Some, such as electrician, have specified visual requirements in terms of colour deficiency on the part of the patient which optometrists may be required to test for and certify. In jobs where colour matching is important, for example a printer, dentist, spectacle frame designer (figure 4) or ocular prosthetic specialist, tints are to be avoided perhaps. This may even include contact lens handling tints. When a tint is required for such a task, for example a train driver or aeroplane pilot, then it must conform to specific standards.
 Figure 4: Tints are to be avoided for tasks involving good colour definition
Figure 4: Tints are to be avoided for tasks involving good colour definition
Working distance
One of the features that differentiates a qualified eye care practitioner from an optical assistant is an understanding of working distance and its relationship to amplitude of accommodation and spectacle lens addition. A senior ABDO examiner, qualified both as an optometrist and dispensing optician, once informed the authors that ‘you will never truly understand presbyopia until it happens to you’. To an extent that is true. However, with some careful thought and a few rules of thumb, it is perfectly possible to understand the problems associated with presbyopia fully.
In simple terms, the maximum working distance, or at least the far point, is the reciprocal of the reading addition. So, a young emmetrope with no accommodation has a far point at infinity, as does a corrected ametrope or a presbyope corrected for distance only since the add is 0.00DS.
An advanced presbyope, with an add of +2.50DS, would have an artificial far point of:
1/2.50 = 0.4m = 40cm
Note that this applies regardless of their overall reading prescription as it is entirely dependent upon the add. It should further be noted that this ignores any depth of field. Small pupils, high contrast subjects and high levels of luminance can all increase the effective range of clear vision. When manufacturers of occupational lenses that have an add of +0.50DS at the top claim a working distance of 4m (rather than 2m), it is this they are depending upon in order to make this claim.
A simple heuristic (‘rule of thumb’) to estimate what add is expected at a certain age is ‘+0.50 for every five years past 35 until aged 60’. Optometrists might refer to this as the ‘tentative’ addition before they determine it accurately.
It should be noted this only really applies approximately to emmetropes, for reasons covered in previous articles myopes tend to become presbyopic later and hyperopes earlier than emmetropes. Nevertheless, table 1 is a good guide as to what should be expected for a working distance of 40cm and significant deviation other than that explained might be cause for concern.
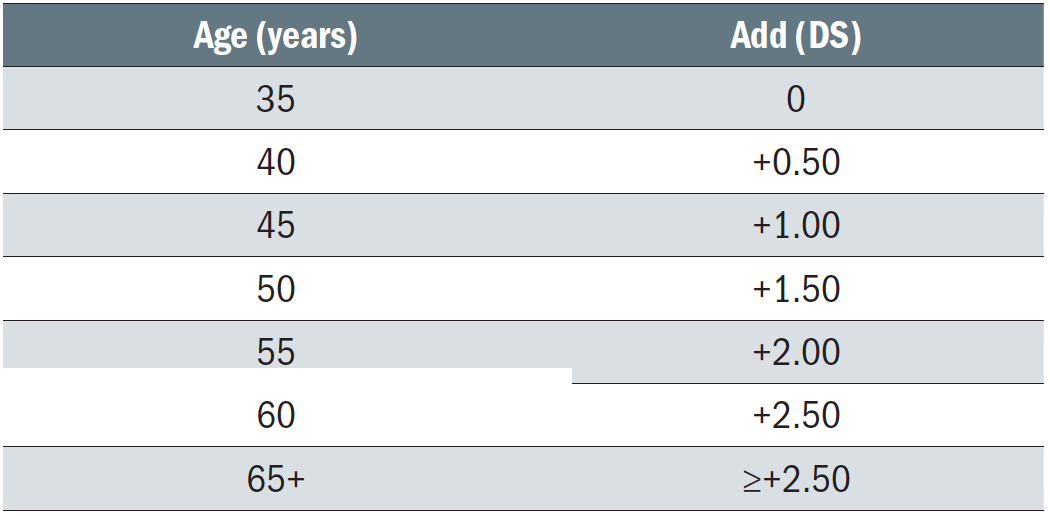 Table 1: Tentative reading addition and age
Table 1: Tentative reading addition and age
The patient’s height may also help to determine their reading addition or accommodation requirements. Shorter patients have shorter arms and will tend to hold close work closer than their taller counterparts. But even if this were not the case, the fixed position of many workstations, whether they be office desks, factory production lines or shop counters, also imposes different working distances for patients of different heights.
For example, the authors are 1.83m and 1.63m and, when working in their kitchen, use the same worksurface which is 93cm above the floor. Measurement shows their respective working distances to be 80cm and 60cm, therefore requiring the differing levels of near vision effort of 1.20DS and 1.67DS respectively. In other words, a taller person may require 0.50DS less accommodation and/or addition to see the same task clearly and comfortably.
Range of vision
Range of vision is also an important consideration. How close a patient can see clearly relative to their artificial far point through a particular addition is dependent upon their amplitude of accommodation. In the authors’ experience, very few optometrists measure (or at least record) amplitude of accommodation. However, it is useful to know this when dispensing in order to determine what proportion of available accommodation is being used during exacting near vision tasks. This is because it is widely accepted that we can only use between 1/2 and 2/3 of our accommodation for protracted close work to be undertaken comfortably.
A young child has around 20.00DS of accommodation (and therefore a near point of 1/20 = 0.05m = 5cm) and this reduces throughout life to effectively zero by the time we reach our 80s. In the absence of individual patient information, the dispensing practitioner must again rely on a rule of thumb (table 2).
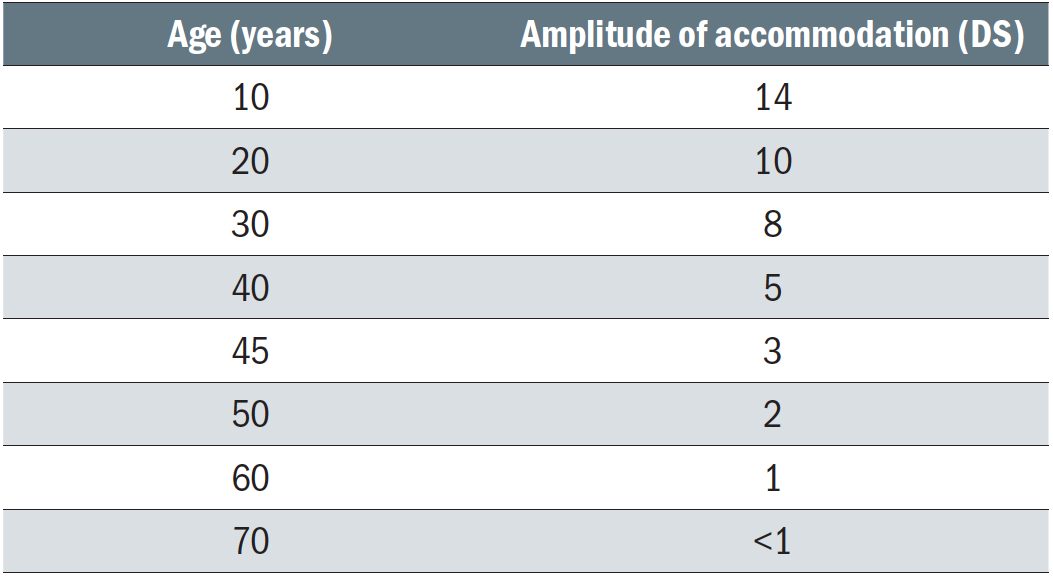 Table 2: Approximate amplitude of accommodation for a given age
Table 2: Approximate amplitude of accommodation for a given age
The far point of the uncorrected eye is simply the reciprocal of the refractive error; 1/F. Hence a myope (without significant astigmatism) will often prefer to read without their spectacles on. A myope of -3.00DS has a far point of one third of a metre, -2.00DS half a metre and so on. This should be made clear to myopes getting contact lenses for the first time, especially if approaching presbyopia. For hyperopes the far point is virtual and is behind the eye. However, they may have sufficient reserves of accommodation, especially at a young age, to place a clear image of a distant object on the retina. That said, their near point of accommodation will be further away than that of an emmetrope exerting the same amount of effort, so near vision is likely to be a problem even if distance vision is not. So, the older the patient becomes or the closer and more exacting the near vision task may be, the more likely this will be an issue.
In practice, we are generally concerned with patients whose distance vision has been fully corrected and therefore have a far point of infinity. The closest point they can see in their distance prescription is effectively their near point of accommodation and is equal to the reciprocal of their amplitude of accommodation. Their closest point for comfortable sustained close work is the reciprocal of half to 2/3 of their amplitude.
Considering a 50-year-old, and referring to tables 1 and 2, we would expect that, when wearing their distance correction, they might achieve a range of comfortable vision from infinity to 1m, perhaps 75cm if 2/3 of their 2.00DS accommodation is exerted, and short tasks at 50cm with maximum accommodation.
Now, imagine the 50-year-old wearing their reading spectacles with an assumed +1.50DS add. The artificial far point here is 1/1.50 = 0.667m or 66.7cm. We can see how this overlaps nicely with the performance of the distance spectacles. In other words, a 50-year-old with average add and amplitude would likely be quite happy with bifocals since they have sufficient
accommodation to see at all distances.
However, consider the same average patient a few years later when their amplitude has dropped to perhaps 1.75DS and the add has increased to +1.75DS. In theory, because the near point of accommodation and artificial far point are the same (1/1.75 = 0.57m = 57cm), the patient would be able to see clearly at all
distances from infinity to their near point using the addition. However, remembering that only half to two-thirds of accommodation can be used comfortably, say +1.00DS in this case for sustained periods, in practice intermediate distances (here closer than 1m to 57cm) become a problem for almost all presbyopes wearing two separate pairs or bifocals in their early fifties.
The artificial far point is an important concept when trying to visualise what the patient will experience when adapting to spectacles that incorporate some form of reading addition. Table 3 shows a selection of reading additions currently available in ophthalmic lenses and the artificial far point associated with each. Adds currently range from +0.40DS in digital add boost lenses (aimed at pre-presbyopes struggling with small print on digital devices) to +25.00DS in high add bifocals (aimed at low vision patients and people engaged in intricate detailed work such as watchmaking or the engraving of jewellery; see case study 1).
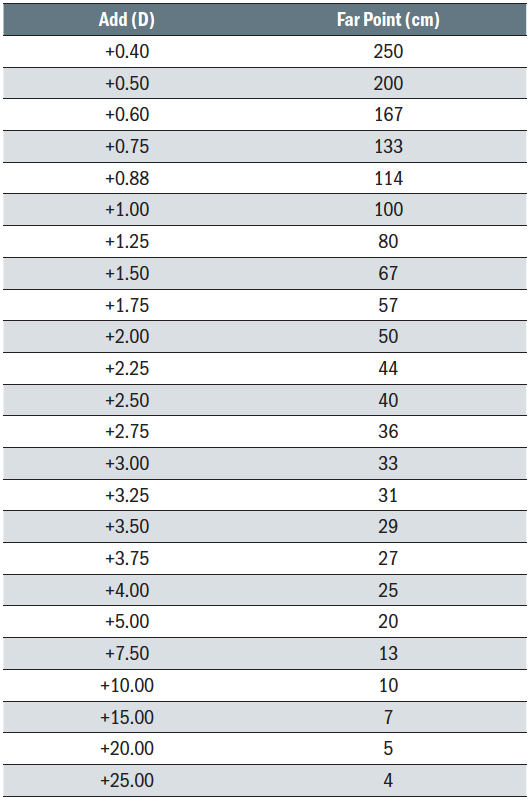 Table 3: Add power and artificial far point for a range of reading additions available in multifocal spectacle lenses (other adds are available including 0.37, 0.53, 0.62, 0.65, 0.82, 0.85DS; please consult availability index of Ophthalmic Lens Availability (ABDO) or manufacturer’s technical information for more details)
Table 3: Add power and artificial far point for a range of reading additions available in multifocal spectacle lenses (other adds are available including 0.37, 0.53, 0.62, 0.65, 0.82, 0.85DS; please consult availability index of Ophthalmic Lens Availability (ABDO) or manufacturer’s technical information for more details)
Low add boost lenses
A number of manufacturers have introduced low add boost lenses in recent years. These are aimed at 20 to 40-year-olds. Confusingly, these have often been marketed as single vision lenses when patently they are not. Interestingly, several manufacturers provide the lenses in what might be termed as non-standard reading additions. The reasons for this are unclear. It may simply be that these lenses command a lower price point than traditional progressive lenses and therefore are intended to be ‘positioned’ differently in marketing terms. However, at a peer review session a few years ago, the point was raised that, for example, a +0.60DS add is the ideal add for the greatest number of patients to see the floor clearly (or more correctly improve near vision without the floor being blurred; the aim is not especially to see the floor). Similarly, a +0.40DS add enables a clear view of the treads immediately below one’s feet when descending steps or stairs. A +0.85DS add allows clear vision of the floor and the whole of a traditional office desk when in the seated position. Whatever the add, from +0.40DS to +1.25DS, digital lenses provide an affordable boost to near vision tasks and easy adaptation for immediate pre-presbyopes and younger adults with insufficient accommodation when viewing small print on hand-held and laptop type display screen equipment.
There is, however, an issue with low add boost lenses that may explain why they are marketed as single vision. If a patient has a prescription for distance only, can a dispensing optician (or optical dispensing assistant for that matter) dispense the lenses and also determine which addition is best? Opinions differ. However, the authors’ opinion is that, if a dispensing optician can determine the addition for the jeweller in Case Study 1, then why would they not be able to determine the add for a similar pre-presbyope struggling to see their mobile phone?
On the other hand, what if the pre-presbyope was struggling with small near targets because of a decompensating exophoria. In this instance, giving a small addition and therefore reducing accommodation/convergence may make the problem worse. So, the decision to introduce a small add to resolve symptoms that may be asthenopia relies on the dispensing practitioner first checking the records to satisfy themselves about the stability of the near binocular status.
Dispensing opticians are reminded that they should make notes of how they have determined the add and why they are recommending it on the patient’s record. This activity is likely to be beyond the remit of optical dispensing assistants who should instead be instructed what to dispense by a supervising registrant.
Case study 1
A special purpose addition for a pre-presbyopic jeweller
A pre-presbyopic jeweller with significant myopia (~ - 7.00DS R&L) had previously been able to do most close work without his glasses on. -7.00DS unaided is equivalent to an emmetrope wearing a +7.00DS reading addition, so this patient’s far point was 1/7 = 0.14m or 14cm. In his early 30s, he had around +8.00DS of accommodation so, without correction, was equivalent to a myope of -15.00DS. His closest working distance, therefore, was 1/15 = 0.667m or 6.67cm without spectacles. However, he was finding he increasingly had to rely on the jeweller’s eye glass at work where previously he had been able to read most hallmarks, engravings and serial numbers (down to ~N2 font size) unaided. He was also concerned that continually putting his frames up on his head while he viewed hallmarks, watch mechanisms and the like, was contributing to his receding hairline; and this certainly appeared to be the case.
This shows the fonts ranging from N11 to N2 he expected to be able to see.
N11 n10 n8 n6 n5 n4 n3 n2.5 n2
We were able to provide him with a Norville 15mm round segment bifocal ‘watchmakers spot’, which is available in adds from +10.50DS to +25.00DS in 0.50DS steps. Although a +15.00DS add would have more closely replicated his previous situation, by racking up +13.00DS in a trial frame and having the patient view his own jewellery, we were able to determine that a +20.00DS add (-7.00 + 20.00 = +13.00DS) best suited his requirements; to see for distance across the shop, use the distance portion for normal near vision tasks, and the segment for most intricate work, only occasionally having to rely upon a jeweller’s eye glass. It is within the dispensing optician’s scope of practice to determine non-standard additions for either intermediate or extra close working distances. Discussion with the prescribing optometrist is not normally required, though it is of course desirable if
convenient.
Display screen equipment
With the widespread introduction and use of computers in the workplace in the late 1980s, experts in ergonomics and health and safety quickly recognised a variety of issues relating to workplace productivity and employee wellbeing. While computers are, in theory at least, labour saving devices, this is only true if they can be used efficiently. Workstation design forms a key part of ensuring productivity and also ensures that employees do not suffer long term health issues. Although initial concerns that display screens may prove harmful to the eyes were unfounded, musculoskeletal disorders, often exacerbated by poor visual acuity or poor posture resulting from inappropriate working distances, means that the Health & Safety (Display Screen Equipment) Regulations 1992 remain in force (and post-Brexit still includes EU Council Directive 90/270/EEC currently under review). Understanding these regulations forms an important part of optometric practice. (see www.hse.gov.uk/msd/dse).
Essentially, employees who use display screen equipment (DSE) daily for at least an hour at a time can request regular ‘eye and eyesight tests’ or their employer can ask them to have same if experiencing difficulties. If the test determines that a special corrective appliance is necessary, and that the normal corrective appliances cannot be used, then the employer should provide a basic appliance appropriate for the work being done. In practice, this means employers pay a basic amount for single vision spectacles in a basic frame, perhaps with an anti-reflection coating, and the employee can pay the difference if they wish to ‘upgrade’ to nicer frames or more serviceable lenses such as degressive enhanced reading lenses or occupational progressive lenses.
Case Study 2
DSE spectacles
Figure 5 shows a not untypical workstation adopted during the home working situation forced by Covid-19. Here, a laptop is connected to a large (34’) gaming monitor that has software to split the screen automatically into two, three, four, six or nine windows and can display four pages of A4 side by side at 100% magnification. Sometimes, during Zoom calls, webinars, or Microsoft Teams meetings, the monitor is raised even further by 10 to 15cm and the laptop is positioned in front of it, behind the separate keyboard, so the camera and microphone can be accessed. While the user has several pairs of personalised progressive lenses, the requirement to see clearly at eye level at a distance of ~75cm was causing significant neck/shoulder discomfort.
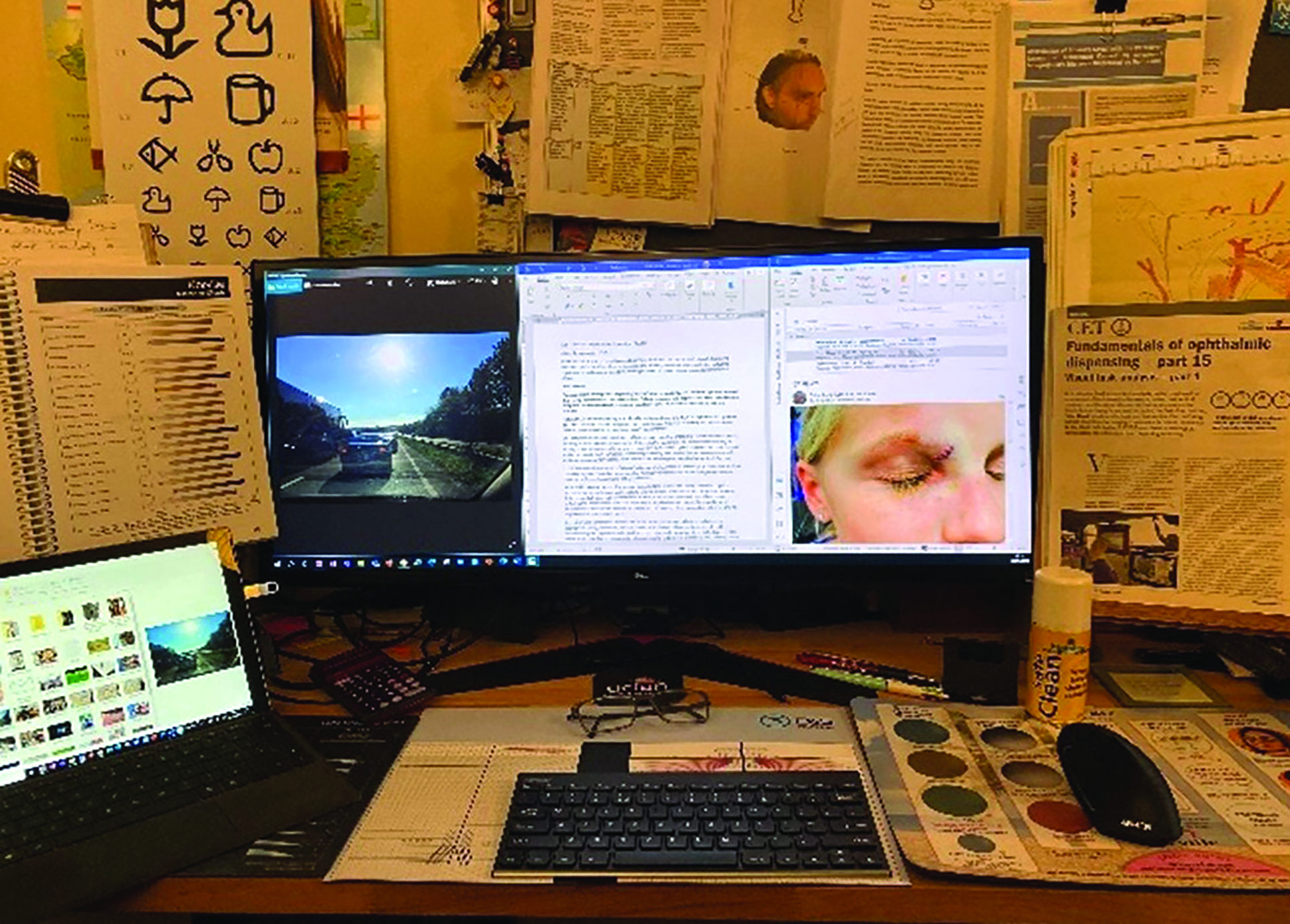 Figure 5: A not untypical home workstation
Figure 5: A not untypical home workstation
A number of options were considered since there is also a requirement to read text and see the keyboard clearly at a distance of ~50cm. These included bifocals or progressive lenses with intermediate at the top (a +1.25 Add) and near (+2.00 Add) at the bottom, and a variety of occupational lenses. In the end the employer funded option of single vision intermediate spectacles was chosen and has proved excellent enabling the user to see all parts of the large monitor, laptop screen, notice board and side document holders perfectly clearly. Although the keyboards are not quite clearly focused, they can be viewed adequately for the task in hand, as can print down to about N6 font size.
Single vision intermediate, or perhaps an old pair of readers, might well be the very best solution for a lot of patients in this situation who currently wear progressive lenses and DSE operators should be encouraged to claim their entitlement in addition to purchasing everyday spectacles so they can appreciate the benefits for themselves.
The DSE regulations specifically exclude displays in vehicles, heavy machinery or any form of transport, as well as portable equipment or small displays such as cash registers or scales. The current review of these regulation needs to reflect the visual difficulties now encountered due to the increased use of screens in these situations. This should be an area of concern for our professional bodies in the UK if we are not to be left with the old regulations when the EU moves on. Driving and the use of machinery will form part of the next article in this series.
Occupational lenses
The term ‘occupational lenses’ tends to refer to lenses aimed at presbyopes. They may be recommended to improve intermediate vision, of computer screens for example, either in terms of focus or field of view, or to address a need to view a task at a close working distance in an unusual direction of gaze, often in combination with other distances in other directions. Like the watchmaker’s spot (Case Study 1), some lenses are aimed at specific occupations. For example, ‘pilot’ lenses have intermediate or near segments at the top as well as the bottom of the lens to accommodate the huge amount of instrumentation found in an aircraft’s cockpit (figure 6).
 Figure 6: The world’s first mother and daughter commercial pilot team need to be able to see clearly at near and intermediate in a variety of directions of gaze
Figure 6: The world’s first mother and daughter commercial pilot team need to be able to see clearly at near and intermediate in a variety of directions of gaze
The simplest occupational lenses are single vision intermediate spectacles and, as Case 2 shows, the benefits are not to be underestimated. However, the author also invested in an additional pair of degressive lenses with an 0.75DS degression and can confirm that, without doubt, they are the best option, allowing clear vision of the workstation in every direction of gaze and the ability to read even the smallest print. Another option would have been to use bifocals with the top portion of the lens set for intermediate and the bottom for near vision. Patients are usually very happy with this option in the authors’ experience.
Perhaps the most undervalued and underused of all ophthalmic lenses are those that we commonly refer to as ‘occupationals.’ These are:
- Degressive enhanced reading lenses
- Vocational progressive power lenses
These two lens designs may have similar outcomes for some patients. However, they have very different design philosophies and also command quite different price points, with enhanced readers being somewhat lower in price. So, it is important to be able to understand the relative benefits of each for a given patient and to be able to explain this to them.
Degressive lenses are, essentially, a single vision reading lens that starts to get less plus above the optical centre and gets progressively weaker towards the top by an amount of degression that is pre-specified. Commonly, 0.75DS and 1.25DS are found but 1.75DS and 2.25DS are available from a few manufacturers. The right and left lens have the same design and the degression is often specified according to the reading add (especially by optical assistants), with adds under 2.00DS having the 0.75DS degression and adds of 2.00DS or more having the 1.25DS degression. Lenses are glazed according to standard near centration distance and centred vertically 3 to 5mm below pupil centre. Some manufacturers once stated ‘to be glazed on HCL’. However, they were actually referring to the facial measurement corresponding to the lower eyelid not some random place that varies with frame style.
Occupational progressive lenses are designed and ordered similarly to general purpose progressives, with a specified distance prescription (usually), reading addition along with distance mono-centration details and monocular heights to pupil centre. Like enhanced readers, unless they are of a bespoke design, they are manufactured to be fitted into frames that have a pantoscopic angle of 8º to 10º so that the centre of rotation condition is satisfied. Occupational progressives are available in a wider range of lens materials and powers and, above all, are available in a full range of adds from +0.75DS to +3.50DS. When the lenses arrive, they will have a ‘distance’ prescription that corresponds to the intermediate requirements specified. For example, a room distance lens (range up to 400cm) might be expected to be +0.50DS stronger than the patient’s distance prescription at the top.
There is now a huge selection of vocational progressive lenses available and it is important to offer a range of lenses that includes a representative sample to satisfy patients’ many and varied occupational needs. It is essential to be fully familiar with the vagaries of manufacturers’ measuring, ordering and verification processes that are frequently different and can lead to careless mistakes. Over the years, marketing departments have shown repeatedly that, when enhanced readers and occupational progressives are offered at deeply discounted prices, uptake is predictably high. But what was also demonstrated was satisfaction levels that are almost too good to be true.
For presbyopes, vocational progressive lenses really do solve a multitude of problems, including those met by presbyopic opticians and optometrists. It is rare to hear of buyer’s remorse when the lenses are purchased as an alternative to single vision reading glasses or as a supplement to general purpose progressives. With personalised freeform occupational lenses, the ability to tailor the intermediate addition, corridor length, height and reading addition to the exact needs of the patient and their task virtually guarantees success, even where needs are complex. Despite this, they remain far from being ‘go to’ lenses for many people and patients are being let down as a result. This may be due to a lack of training, confusion about measurement and ordering, or some difficulty classifying the lenses neatly on practice computer systems. Whatever the reason, there are now several hundred occupational lenses available in the UK, not just from the usual major multinational manufacturers, but also from national and/or independent labs. The products of the latter are often surprisingly ingenious by comparison, as these smaller labs are often adept at satisfying the needs of patients with very specific task-related requirements.
Conclusion
From pre-presbyopia add boost lenses, through degressives and vocational progressives to traditional segmented lenses, there is almost always a solution for every problem if only we are prepared to try. In the next article we will look principally at outdoor tasks and at protective eyewear including filter tints and safety spectacles, as well as at a few lenses with segments.
Peter Black MBA FBDO FEAOO is senior lecturer in ophthalmic dispensing at the University of Central Lancashire, Preston, and is a practical examiner, practice assessor, exam script marker, and past president of the Association of British Dispensing Opticians.
Tina Arbon Black BSc (Hons) FBDO CL is director of accredited CET provider Orbita Black Limited, an ABDO practical examiner, practice assessor and exam script marker, and a distance learning tutor for ABDO College.
Useful Resources
- Ophthalmic Lens Availability 2018, P Gilbert, ABDO
- www.hse.gov.uk/msd/dse