Patients often lead quite complex lives from a visual stand point, and two standard questions, asked by optometrists with regard to vocational requirements; ‘do you drive?’ and ‘do you use a computer?’ are now so universally answered in the affirmative as to be almost surplus to requirements.
As previously discussed, asking what someone does for a living is also less than revealing in terms of the visual nature of their work and a better question might be to ask what their job role involves from a visual standpoint. Even so, the nature of people’s busy lives means it is hard to get to the detail of a patient’s visual needs without spending some considerable time and it is perhaps best done more fully as part of the dispensing process. For example, the authors are acquainted with a presbyopic forensic scientist whose job requirements include:
- Driving
- Global travel
- Extensive use of a variety of electronic devices
- Presentations and teaching
- Laboratory work; requiring safety spectacles with highly detailed near vision
- DIY
- Wood-chopping; for his wood burning stove
- Going to the gym
- Swimming
- Running
- Cycling
- Badminton
Clearly a difficult case to satisfy with one pair of spectacles. Although dispensing multiple pairs of spectacles to patients is an aspiration of most business-focused practices, the training of opticians tends to focus on case records that present only one problem. During their training, dispensing opticians, for example, prepare case records relating to sports, or tints, or safety eyewear, or high-powered lenses say. There is a tendency to treat the patient as an ocular condition or lens type (for example as an aphake, a gross anisometrope, a bifocal or progressive lens wearer) yet a patient could be almost any combination of these things and more.
 Figure 1: It is easy to ignore routine outdoor tasks such as dog-walking
Figure 1: It is easy to ignore routine outdoor tasks such as dog-walking
It is important to see the person as a whole, not just attempt to satisfy their basic requirements or to base your advice simply on what they have had before. Asking a patient if they have been happy with their previous glasses either yields an unproductive ‘they were fine until my eyes changed’ or opens a can of worms that the optician would rather have kept closed. It may be better to ask, ‘could anything have been improved about your old glasses?’ This is more likely to encourage the satisfied to suggest improvements and the dissatisfied to focus on the key issues.
It is easy for both practitioners and patients to forget about routine everyday outdoor tasks, such as dog-walking, gardening, or relaxing outside, and concentrate on more determined outdoor activities such as sport, exercise or work-related activities.
Glare
Glare reduction
Many patients with clear lenses are troubled by bright light in sunny weather. Discomfort glare, although not actually harmful, can cause a person to narrow their palpebral aperture (figure 2) in order to see comfortably which can lead to fatigue and headaches and may even contribute to earlier onset of the temporal skin wrinkles known as ‘crow’s feet’.
 Figure 2: Discomfort glare can cause a reflex narrowing of the palpebral aperture
Figure 2: Discomfort glare can cause a reflex narrowing of the palpebral aperture
Many patients will find it beneficial to wear photochromic lenses (figure 3). Others, especially if they are outdoors for longer periods, may prefer a fixed or polarising tint (figure 4). Photochromic lenses are improving by the year, nevertheless they do not react instantaneously, especially in terms of fading when the wearer moves indoors, and it is important to set patient expectations accordingly. Patients who often find themselves in warmer climates often complain that their photochromic lenses do not go dark enough, whereas patients in cooler climes may complain that the lenses go too dark in cold but dull conditions. This temperature dependency is to be expected, although performance varies considerably between available options, and again it is important to set expectations. When patients complain about photochromic lenses the typical response it either to move the patient back to clear lenses or to swap the photochromics for a fixed tint lens.
 Figure 3: Photochromic lenses offer UV protection and excellent glare reduction
Figure 3: Photochromic lenses offer UV protection and excellent glare reduction
 Figure 4: In brighter conditions, patients may prefer a fixed tint, here shown in clip-on form
Figure 4: In brighter conditions, patients may prefer a fixed tint, here shown in clip-on form
In reality, it may be better to recommend two separate pairs. For the patient who does not find them dark enough on occasion, recommend keeping their photochromics and having an additional pair of prescription sunglasses. For the patient who finds the winter months ‘depressing’, a clear pair for use when the weather is cold and dull but the available UV radiation (which causes the photochromic reaction in most cases) is high.
Veiling glare
While discomfort glare is tiring and uncomfortable, veiling glare can be inconvenient, even dangerous, since, as the name suggests, the glare can hide from view what lies beyond. Veiling glare is a particular problem for anglers. Course fishing often involves focusing on a tiny float at a distance of 10 metres or more against a background of light reflected from the surface of the water and, while leisure anglers have choice of where to fish, competitors in match fishing have no such choice and could find themselves drawing a peg opposite a low sun or bright sky reflecting from the surface. Fly fishing for species such as trout and salmon is in the clearest of waters and the removal of reflected glare from the surface of the water is very helpful in locating fish. There is only one option for fishing in bright conditions and that is polarising lenses. For float fishing the enhanced contrast afforded by brown lenses is preferred by many as the fluorescent orange/yellow/red of the float is more highly visible.
The authors have often heard it said (typically from students in exams) that polarising lenses are banned for fishing, especially competitive match fishing, however, they can find no record of this rule at national or international level. While one can never be sure of local rules or those of individual private fisheries, would urge practitioners to advise of the benefits of polarising lenses to all patients who have cause to spend time near water. Polarising lenses are widely discussed in the angling press, on TV and in social media so contradicting such influential advice can make practitioners look ill-informed and out of date.
Case study; angling
It is easy to assume that all patients who list fishing as a hobby have the same visual needs, however, with the exception of UV, protection and glare reduction needs can vary quite dramatically, especially for near vision. Competitive match fishing often involves catching large numbers of tiny fish using lines as fine as 0.06mm diameter (340grams breaking strain) and hooks with a gape of less than 2mm (figure 5), which must be tied securely and removed from fish safely, all of which requires excellent near vision. To put this in perspective the fishing line all opticians are familiar with is the #8.0 0.5mm nylon monofilament used as supra cord – which at nearly 10 times the thickness of the finest lines has a breaking strain tested to 18.4kg which is not untypical for sea angling.
 Figure 5: Fishing hooks come in huge variety of sizes for catching everything
Figure 5: Fishing hooks come in huge variety of sizes for catching everything
from the tiniest freshwater species to the largest sharks
Fishing also presents a variety of safety issues in addition to UV exposure. Casting out, especially in windy conditions and with lightweight tackle, exposes the angler, or anyone nearby to the possibility of being ‘hooked’. Such injuries are surprisingly common and if they occur in the eye can be very serious (see figure 6). Not only would a hook introduce a host of potentially dangerous pathogens into the eye, most hooks used in disciplines of the sport where the fish are not normally returned to the water but kept for food, are barbed in nature and designed to not easily come out. The advice for skin injuries is to snip off the eye of the hook and feed the hook through to exit the skin at a different point so that it is not forced backwards against the barb. Clearly when the eye is involved this is a delicate operation and will require anaesthetic so first aid might involve removing any other tackle so no weight is attached and taping any remaining line/tackle to the face, and padding the eye to immobilise it.
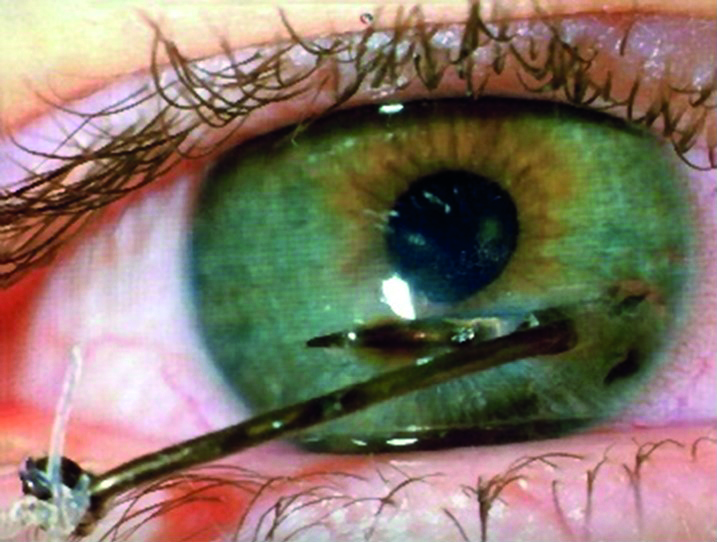 Figure 6: Barbed hooks are designed not to come out so ocular fish-hook injuries can be very serious
Figure 6: Barbed hooks are designed not to come out so ocular fish-hook injuries can be very serious
A further risk when fishing is becoming snagged in rocks or weed. In an effort to free the hook/tackle, considerable force can be exerted and when the tackle breaks free, if the line has not broken then the hook and weights will fly back towards the angler at incredible speed with potential for considerable injury especially to an unprotected eye. Safety is therefore an important consideration. Any close fitting frame will deflect an errant hook so standard frames fitted with plastic lenses should be recommended as a minimum, however, the use of heavyweight tackle as is the norm in sea angling and carp fishing should indicate protective eyewear with polycarbonate or Trivex lenses. Industrial safety eyewear will be covered in a future
article.
Many anglers appreciate the benefits of separate prescription polarising sunglasses, others are very happy with flip-up polarising clip-ons as they are easier to manage. Accessories to keep the frame in place are also important as slippery surfaces are common and there is considerable risk of losing the spectacles in the water – it is even possible to provide floats to avoid them sinking (figure 7).
 Figure 7: Floats are a useful accessory for anglers, rowers and anyone else at risk of losing their spectacles in water
Figure 7: Floats are a useful accessory for anglers, rowers and anyone else at risk of losing their spectacles in water
Outdoor activities
Bird and wildlife-watching
The authors live in West Lancashire close to the Wildfowl and Wetlands Trust at Martin Mere (figure 11) and are often aghast at the expensive optical hardware, whether it be telescopes, binoculars or cameras with huge telescopic lenses, they witness birdwatchers using. Many have good optical knowledge and are highly appreciative of the benefits of antireflection coatings, photochromic and polarising lenses, and also the fact that one appliance is rarely the solution to all problems. However, others, no less passionate about birds, are less knowledgeable about their optical options.
 Figure 11: Geese over Martin Mere. Birdwatchers are often highly knowledgeable about the benefits of optical products but not necessarily so. Digital photography requires excellent near vision as well as distance vision to ensure that the final image is clearly focused
Figure 11: Geese over Martin Mere. Birdwatchers are often highly knowledgeable about the benefits of optical products but not necessarily so. Digital photography requires excellent near vision as well as distance vision to ensure that the final image is clearly focused
A simple thing to check if they wear glasses is that they have binoculars with a retractable eyepiece cup (usually made of flexible rubber that can be folded back) which enables the binoculars to sit at the correct point before the eye when used with spectacles to give the correct eye relief to position the exit pupil correctly and maximise field of view. Adjustable eye relief is a feature of most binoculars, telescopes and hand-held telescopic low vision aids, however patients whose use of binoculars/telescopes pre-dates their use of spectacles may be unaware of how to get the best from them. Figure 12 shows two identical telescopes (for low vision use) one with the eye relief set for an emmetropic patient, the other with the eye cup folded back for use with spectacles.
 Figure 12: Binoculars and telescopes usually have retractable eye-piece cups that for an emmetrope are placed against the orbital rim (left),
Figure 12: Binoculars and telescopes usually have retractable eye-piece cups that for an emmetrope are placed against the orbital rim (left),
but for spectacle wearers need to be folded back (right)
Patients using optical devices such as binoculars, telescopes or optical microscopes that come into contact with their spectacle lenses will find a scratch resistant coating is essential and an anti-reflection coating of great benefit.
Eye relief is a term used to describe the distance from the outer surface of the eyepiece lens to the position where the exit pupil is formed (eyepoint), approximately 3mm behind the corneal surface. Looking through binoculars from the eyepoint, you can obtain the whole field of view without vignetting (figure 13a). Using the same binoculars with spectacles results in a vignette of the original image, a narrower field of view due to the longer eye relief (figure 13b). However, folding back the eye-cups to restore the original eye relief facilitates maximum field of view when wearing spectacles (figure 13c).
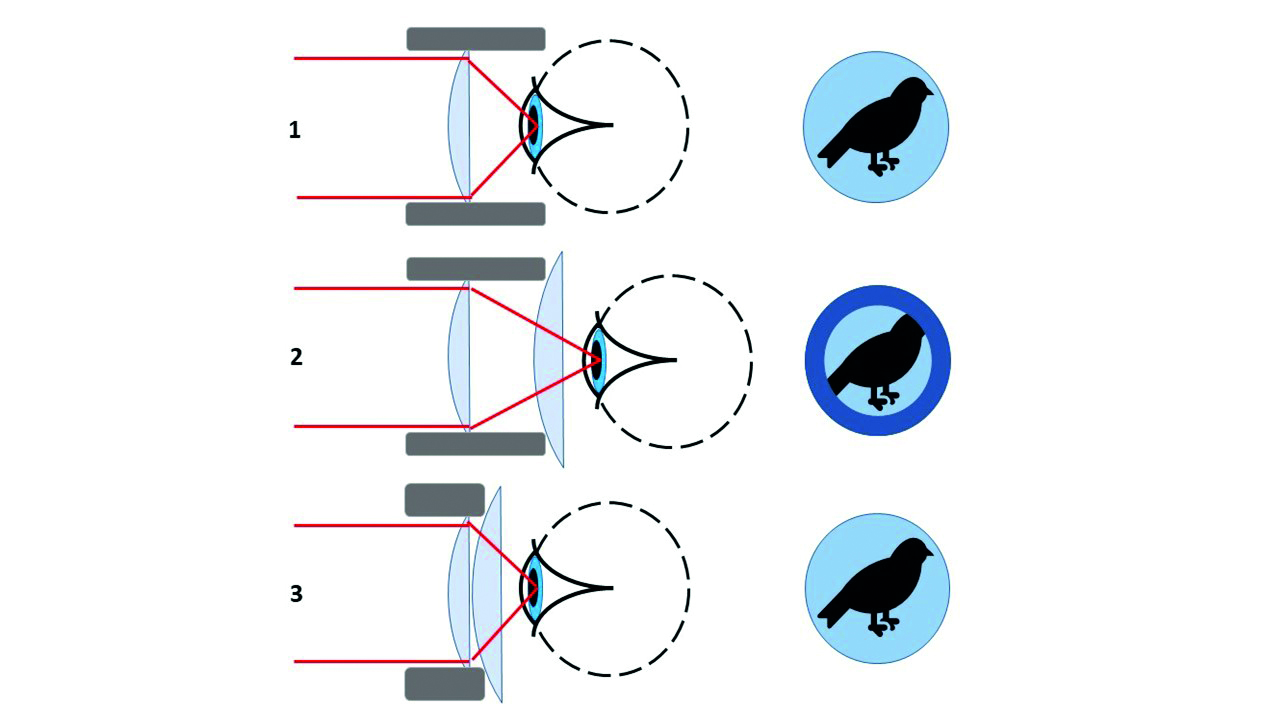 Figure 13: The effect of retractable eyepiece cups in restoring the eye relief and field of view experienced by emmetropes when a spectacle wearer uses binoculars or a telescope
Figure 13: The effect of retractable eyepiece cups in restoring the eye relief and field of view experienced by emmetropes when a spectacle wearer uses binoculars or a telescope
Digital photography
Photography poses a particular challenge to the presbyope. The days when a photographer took a picture and forgot about it until it was developed are long gone and clear near vision is also important checking the composition and clarity of a shot before potentially trying again. Another feature of digital devices, including cameras, sat-nav screens and some phones, is that their screens will more than likely emit plane polarised light, which is completely eliminated by polarising sunglasses in at least one orientation.
Driving
The most common experience of veiling glare is when driving. Evidence suggests car accidents increase by around 16% in sunny weather when disabling glare is present. Glare is most troublesome on roads that run east to west when the sun is low in the sky – an hour after sunrise if travelling east, and an hour before sunset if travelling west. When these hours coincide with the daily morning and evening rush hours the problem is at its highest – which in the UK is not during the summer but instead October and February. Veiling disability glare is exacerbated by windshields being dirty both inside and out causing light scatter (figure 14) and patients should be advised accordingly – patients sometimes return polarising lenses as being ineffective and are disbelieving that traffic film or nicotine on the inside of the windscreen is part of the problem if not warned in advance.
 Figure 14: Blinding disability glare is exacerbated by dirty windscreens
Figure 14: Blinding disability glare is exacerbated by dirty windscreens
Veiling disability glare is at its worst when driving when the low sun is reflected from a wet road, however reflections from inclined surfaces, such as solar panel arrays or the back window of the car in front, mean disability glare can strike at almost any time in bright conditions. Motorcyclists (figure 15) suffer similar problems with the added challenge that any frames dispensed must fit together with a helmet. The best option for most people is a polarising lens (figure 16), which greatly reduces the reflected light (since it is plane polarised) as well as absorbing a significant percentage of the ambient light across the visible spectrum. Polarising lenses are available in a wide variety of colours and depths, however, are most commonly dispensed in either brown, grey or green with visible light transmission of around 25 to 30%.
 Figure 15: Motorcycling poses similar visual challenges to driving with the added complication of
Figure 15: Motorcycling poses similar visual challenges to driving with the added complication of
ensuring frames can be put on and taken off while wearing a helmet
 Figure 16: Polarising lenses greatly reduce reflected veiling glare when driving
Figure 16: Polarising lenses greatly reduce reflected veiling glare when driving
Standards relating to driving
When supplying tinted sunspectacles it is important to inform the patient of the limitations of wear and ensure they are fit for the intended purpose. In particular BS EN ISO 12312-1:2013 (Eye and face protection – Sunglasses and related eyewear – Part 1: Sunglasses for general use) applies to all prescription and plano sunglasses (including clip-ons) except those used for direct observation of the sun (which are covered in part 2 of the standard). It also includes photochromic spectacles.
When supplying any tinted lens it is important to inform the patient in advance on any limitations on use relating to driving. In particular this relates to the use of tinted lenses in dim light conditions. Section 5.3.2.4 states that lenses incorporating a filter of ‘luminous transmittance of less than 75% shall not be used for road use and driving in twilight’. It is important to note that this cut-off point of 75% visible light transmission is at odds with the category values within the standard when it is generally taken that category 0 tints are suitable for driving in all light conditions, category 1, 2 and 3 in daylight conditions, and category 4 are not suitable even for daytime driving. In fact the palest category 1 tints are also suitable for night driving providing visible light transmission exceeds 75% which is just as well as a large proportion of uncoated general purpose photochromic lenses in their faded state, especially those made from glass materials, would not be suitable for night driving otherwise without an antireflection coating (which is a wise addition in any event). Table 1 attempts to clarify the issue.
BS EN ISO12312-1 also lays out many other requirements that the sunglasses and filter lenses we dispense must meet, including: the uniformity of tint (which effectively precludes the sale of solid tints in all but the lowest of prescriptions); performance of photochromic lenses; and axis of orientation and efficiency of polarising filters.
In addition to table 1, there are several other requirements relating to road use and driving. These include a requirement that between 475nm and 650nm the spectral transmittance should be no less than 0.2τv and that the lens should not impede the recognition of red, yellow, green and blue signal lights within specified relative visual attenuation quotients. As a result a number of quite pale tints are unsuitable for driving under any circumstances and these include purple, pink/red and blue tints. When recommending a tint other than the standard brown, grey or green grey colours do be careful to check suitability for driving and if your practice lacks suitable measuring equipment order tinted lenses, of a specified transmittance profile, from a reputable supplier, rather than relying on a random dip dying process in practice.
Case study; an illegal tint?
Mrs J was going on holiday and had called to collect her prescription sunglasses the day before only to be told that they were not ready. A rush job was required so that she could collect the next morning, lenses were obtained from a nearby practice, edged and towards the end of the day placed in the tint bath. As a level 3 tint of 15%LT was required this would take quite a while and unfortunately the technician forgot about them before going home. The next morning as the patient arrived first thing it was realised that the lenses were still in the tint bath, which although it had been switched off had continued the tinting process as the tinting dyes cooled. Although darker than the practice sample there was not time to bleach the lenses as the patient was on her way to the airport. The lenses seemed OK to the technician and the dispensing optician so the glasses were quickly assembled and fitted to the patient.
Some weeks later a solicitor’s letter was received following the patient’s involvement in a serious road traffic accident and placing the blame on the sunglasses being too dark. Subsequent scientific evaluation of the spectacles revealed visible light transmission of less than 6% – a clear category 4 filter which should have been accompanied by a warning not to use for driving (except, according to BS 12312, possibly in extreme high luminance conditions such as desert or snowfields in full sunlight). Fortunately the patient recovered from her injuries and her car and the parked car she hit were fully insured and she settled out of court with the practice’s insurer. However, this could easily have been more serious – it is not difficult to imagine a case of gross negligence or corporate manslaughter under these
circumstances.
Practices that tint lenses on the premises should invest in appropriate measuring equipment to check that any did dyed lenses they supply conform to standards. Many automatic focimeters have built in visible light and UV meters for the purpose of providing basic information, however more detailed transmission curves are required to be sure of meeting the standards for driving.
Case study; polarising lenses and informed consent
Polarising lenses have some downsides that practitioners must be aware of and must make patients aware of if consent is to be valid and informed and to avoid preventable disappointment and patient complaints. The most common drawback is that many digital displays emit plane polarised light meaning that the light is completely eliminated by an appropriately oriented polarising filter. Most modern LCD displays including smart phones and built-in sat-nav screens have oblique orientation so are not adversely affected, however, with many digital cameras the screen may only be visible in say landscape and not portrait orientation or vice-versa. Patients also need warning that they may notice some unusual effects such as the stress patterns being revealed in toughened glass car windows, and patterns appearing in LCD screens, and should be encouraged to try polarising filters with their devices before purchase.
Some skiers also report that polarising lenses should be avoided since ice patches become less visible if their tell-tale reflections are eliminated which could be dangerous. At CET events, many opticians who ski report no such issues and prefer polarising lenses themselves, and certainly there are plenty of snow goggles available with polarising lenses. However, it is prudent to demonstrate knowledge and understanding by explaining to any prospective purchaser.
Night driving
Driving presents many visual challenges and for many patients their main concern is when driving at night. The gradual move by car manufacturers from halogen, through xenon to LED headlights is seen as a brighter blue-white light compared to warmer yellow-white and many patients complain that they feel glare at night is getting worse. Dirty windscreens, especially on the inside, play an important part, as does the fact that larger pupils at night subject the retinal image to greater coma, spherical and higher order aberrations. In older patients advancing cataracts may be part of the problem and may be cause for early referral if having a significant impact on the patient’s work or quality of life.
Glare from headlights can be significantly reduced with an anti-reflection coating, possibly in combination with a very pale tint. On balance, at night the aim is to maximise the light reaching the retina, however, since the blue-white light is perceived by most patients as the root of the problem it is prudent to select and anti-reflection coating that has a blue/violet residual colour that selectively reflects the problem wavelengths. A pale brown or straw-coloured tint can also reduce blue light significantly and a number of manufacturers have introduced tint/coating combinations (as well as single vision and progressive lens designs) specifically aimed at driving including at night; for example, Optimum inMotion, Lenstec ExDrive, Norville Freeway, Zeiss DriveSafe, Hoya EnRoute, Rodenstock Road, Essilor Road Pilot, etc.
Case study; night-time glare
Mr B has always been troubled by glare when driving at night and after taking a new job found himself driving many more miles per year. Standard lenses with an anti-reflection coating did not make any noticeable difference so it was decided to conduct a refraction using a wave-front aberrometer (used by the practice for pre-operative laser surgery assessment) and order a freeform tailormade single vision lens to correct for higher order aberrations (Zeiss i-Scription) as well as a coating specifically aimed at motorists (DriveSafe).
A few weeks after collection the patient returned dissatisfied, however, while the spectacles were being checked it came out in conversation that the problem did not occur in his wife’s car, only his own. It being a dark winter’s afternoon a short walk to the car revealed the problem. The car had an LCD dashboard display and built in sat-nav that were so bright as to interfere with the eye’s ability to adapt to dark conditions. Once the patient was shown how to change the illumination of the cockpit display (figure 17) to maximise the eye’s scotopic ability, the problem was solved. Mr B was able to compare his new and old glasses and agreed that the combination of personalised single vision lenses and a tint/coating combination specifically aimed at driving was a significant improvement though not quite as useful as making an adjustment to the car itself.
 Figure 17: Many cars with an LCD display or built-in satellite navigation have adjustable displays and even a choice of colour schemes. Dimming the illumination can dramatically improve visual performance under twilight and night-time conditions
Figure 17: Many cars with an LCD display or built-in satellite navigation have adjustable displays and even a choice of colour schemes. Dimming the illumination can dramatically improve visual performance under twilight and night-time conditions
Sport
Many sports pose no significant ocular risk to emmetropes (figure 18). The risk is created by the wearing of prescription spectacles which if struck with force during a fall, or contact with a ball, elbow, head, etc, can cause facial or ocular injury. In such cases contact lenses should be offered as the most appropriate solution for most patients. It may be helpful to remind people that many world class sports stars wear contact lenses (including Novak Djokovic, Cristiano Ronaldo and Katarina Johnson-Thompson) to improve their game.
 Figure 18: Many sports pose little ocular risk unless spectacles are worn
Figure 18: Many sports pose little ocular risk unless spectacles are worn
 Figure 19: Girls have helped make football the UK’s largest participation sport
Figure 19: Girls have helped make football the UK’s largest participation sport
Patients who do not consent to contact lenses should be informed of the risks of playing sport in standard spectacles (or without eye correction altogether as is required by some referees and school sports teachers) and offered appropriate sports spectacles in addition to the patient’s everyday spectacles.
Case study; facial injuries
According to the FA, football is now the largest participation sport in the UK, largely due to the recent surge in interest in girls’ and ladies’ football. Although football remains a relatively low risk sport its contact nature means a stray ball, elbow or finger can cause significant eye injury. At least one child has lost an eye due to lacerations caused by a broken CR39 lens after his spectacles were struck by a football.1
It is interesting to note that in the 40 or so teams that play in the authors’ daughter’s football league on a Sunday morning the players most likely to be wearing spectacles seem to be in goal and are most likely to sustain clashes with other players and the ball. Figure 20 shows an injury sustained by the goalkeeper – it is not clear whether the broken frame or the unbroken lens actually caused the injury, however, the player now wears contact lenses.
 Figure 20: A brow injury caused by an acetate frame that broke on impact from a football
Figure 20: A brow injury caused by an acetate frame that broke on impact from a football
Injuries caused by standard spectacles during sporting activities can be extensive in the authors’ experience. Pad on arm frames can result in a penetrating injury, even a broken nose if impacted with sufficient force, and may even require plastic surgery. Racket sports, particularly squash and badminton, present perhaps the greatest risk of all sports and even emmetropes should be recommended to wear sports eyewear for protection.
At junior level, the authors have observed that, because few children require sight correction and many that do wear contact lenses for sport, spectacles are largely out of sight and out of mind with regards to coaches, referees and umpires who seem not to be aware of the rules. ABDO publishes guidance on sports eyewear including dedicated leaflets on both football and cricket.2 However, much information and the unique rules relating to each sport can be found on each sport’s governing body website, as is the case for such as for football,3 rugby4 and hockey.5
Most games mandate a padded sports frame and plastic lenses. However, it is often left to the discretion of the referee and a quick glance at online forums reveals some very dubious opinions. Children often find themselves allowed to play in their everyday glasses one week, yet another week not allowed on the pitch at all, even with sports goggles, sometimes forced to play uncorrected and so adding to their risk of injury. The best advice is to look up the rules of the game before advising the patient/parent.
For football, the laws of the game are quite straight-forward.6,7 Law 4 relates to the players’ equipment. Under the section labelled ‘other equipment’ the law states that non-dangerous protective equipment (for example, headgear, facemasks and knee and arm protectors made of soft, lightweight padded material) is permitted, as are goalkeepers’ caps and sports spectacles.
Figure 21 shows a variety of frames suitable for football and most other sports excluding rugby, which is currently trialling specific goggles. Within the rules of football, the frames must be fitted with polycarbonate lenses and a head band and, unlike other sports, plano spectacles may be worn for protection only, even if a prescription is not required. This was the case with Dutch international Edgar Davids who had a rare form of glaucoma (figure 22).
 Figure 21: Sports frame suitable for football and many other sports
Figure 21: Sports frame suitable for football and many other sports
 Figure 22: Dutch former international football player Edgar Davids
Figure 22: Dutch former international football player Edgar Davids
Although sports eyewear is intended to offer the best protection available, there is always the possibility that the wearer may sustain an eye or facial injury due to severe impact or because of the nature of the athletic activity. The Football Association (FA) advises referees to ‘ensure that, if a request has been made to wear glasses/goggles, that they must not be a danger to themself or to any other player’.
While recommending polycarbonate lenses, the FA also recognises this may be an issue for children playing in grassroots football. They therefore ‘encourage referees officiating in grassroots youth football to be tolerant over glasses. However, the individual referee has to show concern for all those playing in that game and if s/he feels there is something dangerous in the glasses (such as sharp edges and so on) then, in order to protect players and also the wearer him/herself, s/he has the authority to say the glasses cannot be worn.’
Opticians are often called upon to mediate between children and their schools or sports clubs, so it is incumbent upon all registrants to research the individual requirements of a given sport when a specific patient presents to ensure that the advice given is up to date. It is no longer acceptable for children to be discriminated against and prevented from exercising or participating in sports because they require sight correction. However, it is important that they are informed of their options and the associated risks.
Conclusion
It is easy to think of task analysis as being mainly concerned with computer workstations and industrial safety eyewear, however, every person, whatever their age, has a unique set of requirements relating to work, leisure, hobbies, sports and everyday tasks that barely merit a second thought. It is rare for one pair of spectacles to solve all problems and by adopting a problem-solving approach patients are more likely to see the benefits of their different options.
- Peter Black MBA FBDO FEAOO is senior lecturer in ophthalmic dispensing at the University of Central Lancashire, Preston, and is a practical examiner, practice assessor, exam script marker, and past president of the Association of British Dispensing Opticians.
- Tina Arbon Black BSc (Hons) FBDO CL is director of accredited CET provider Orbita Black Limited, an ABDO practical examiner, practice assessor and exam script marker, and a distance learning tutor for ABDO College
References
- https://www.manchestereveningnews.co.uk/news/greater-manchester-news/manchester-fa-glasses-football-boy-15865147
- https://www.abdo.org.uk/for-the-public/leaflets-about-eyecare
- www.thefa.com
- www.englandrugby.com
- www.englandhockey.com
- https://www.thefa.com/football-rules-governance/lawsandrules/laws/football-11-11/law-4---the-players-equipment
- https://www.teamgrassroots.co.uk/fa-guidance-for-spectacles-and-goggles-in-football