So far in the series, the main focus has been upon the use of existing technology in general use that may be adapted to help those with vision loss. Examples of such assistive technology range from televisions to smartphones, tablets and computers, all of which can be adapted to offer a whole host of options, including magnification, contrast enhancement, audio signalling and so on. As helpful and cost effective as many of these assistive options often prove to be, they still involve the use of technology designed for general purpose use that is somehow adapted for the visually impaired by the use of specialist software or changes to their settings.
In this article, we will take a look at systems that have been designed specifically for the use of the visually impaired and, as such, may be described as adaptive technology. Such systems are usually listed as medical devices, as defined by the UK Medical Devices Regulations 2002 (Amendment EU Exit) Regulations 2020 2, and have been designed and tested for specific use by a target group for whose needs the system is aimed at supporting.1 Such classification may dictate the eligibility of the system for inclusion in NHS funded schemes. This is important as the cost of adaptive technologies can be a major challenge to many who might benefit from their use.
Classificiation of adaptive technology
Classification of low vision aids has become increasingly difficult as devices have evolved. Historically, a distinction was made between simple aids (spectacle, hand and stand magnifiers) and complex aids (telescopes and CCTVs). This somewhat arbitrary distinction was based upon complex aids usually requiring some extra training for the user and the fact they consisted of multi-lens or electronic components.
Closed circuit television systems are those where an image is captured by a camera and displayed on a screen in a way that allows the displayed image to be enhanced in some way. Though there have been overhead projector style devices that are purely optical in design, where a lens is used to magnify the image of an object on an illuminated bed, which may then be projected onto a screen in enlarged form, the majority of CCTVs have relied upon electronic image capture and enhancement. Initially, this was via cathode ray tube technology which made the first CCTV magnifiers bulky, costly and prone to image quality degradation at higher magnifications. With the advent of digitisation, electronic systems have evolved that are much more portable, adaptable and with display technology capable of maximising contrast and resolution at higher magnification levels.
As some electronic magnifiers are designed to mimic optical aids and be as easy to use as possible, for example the portable video magnifier in figure 1, the distinction between simple and complex aids is nowadays less useful. It might be argued that a handheld unit with an autofocus feature might be simpler to use than an optical hand-held magnifier where a degree of positional focusing on the part of the user is required.
 Figure 1: A portable hand-held electronic magnifier
Figure 1: A portable hand-held electronic magnifier
While the term CCTV is still used by many to describe any device where a camera is connected to a display screen of some sort, its generality of usage, for example in security systems or for spying on the Health Secretary, has led to the adoption of a more specific term when such a as system is used for image enhancement for the visually impaired; electronic visual enhancement systems or EVES. This term is increasingly being used in the literature to described electronic magnifiers, though other terms, such as video magnifiers, are still in common usage. The remainder of this article will use the term EVES for the adaptive technologies discussed, but even this is something of a generalisation.
EVES implies visual enhancement, the manipulation somehow of the visual input. Some adaptive technologies use non-visual enhancement, for example the use of auditory input. Image-to-speech systems, GPS navigational devices and those that use auditory signals or vibration representation of the visual world might, in this author’s view, be better defined as electronic perceptual enhancement systems, or EPES. Many of the apps described in the previous feature in this series (Optician 25.06.21) might also be better described as such. That said, most modern EVES are often multifunctional and may combine image enhancement with, for example, an audio input, so rendering precise classification less relevant.
Finally, in recent years, there has been the development of instruments capable of generating their own images to augment the real world. Such augmented or virtual reality systems are considered in this article under their own section.
Adaptive devices for reading text
There is a wide range of adaptive devices capable of capturing the image of text and, instead of enlarging it, reads it out. Such reading machines make it possible for someone with no functional vision to be able to access reading materials.
There are three main types of reading machine:
- Standalone devices; these combine a camera or digital scanner, optical character recognition (OCR) software, and an audio output with or without linkage to a display screen in a single device.
- Computer-based devices; these connect a camera or scanner and OCR software to a user’s computer, allowing them to employ existing screen display options in their computer alongside the audio output from the attached reading device.
- Portable devices; these are lightweight and easy to use and, with the ongoing digital evolution, have become increasingly adaptable in being able to describe, not just text, but other objects as well as offer locational information.
Figure 2 shows a selection of such devices. Dedicated reading machines will read out printed documents using a synthetic voice. This is worth remembering, as not all users take well to such voices, especially if heavily accented. That said, as with GPS systems in cars, voice options are often available to best suit the user.
 Figure 2: A selection of portable and desktop standalone reading machines
Figure 2: A selection of portable and desktop standalone reading machines
As these systems use a scanner or a camera with optical character recognition (OCR) software to convert printed materials into electronic form that can be read out loud by a screen reader, many also offer visual representation and so blur the boundary with other EVES systems.
As has already been discussed in this series, there are many apps that run on standard smartphones and tablets that will provide very similar functionality to the above specialist options and are much cheaper if you already own a smartphone or tablet. Their reliability can vary widely, however.
EVES
Whereas reading machines are designed primarily to offer an audio output, EVES are designed to display a captured image in a way that might be manipulated and enhanced to assist those with impaired but residual functional vision. They tend to be classified in terms of their size and portability as follows:
- Desktop EVES; these offer the highest degree of magnification and most also have greater functionality, such as colour and contrast changes, image capture, audio output, voice control, selective word or image capture and so on (figure 3).
- Portable EVES; these can either be standalone devices or connect to a laptop computer, utilising software on the laptop to control the display, use OCR, or capture and store images of printed text. Some magnifiers enable distance viewing, for example lectures or presentations (figure 4).
- Pocket EVES; these are small enough to use on the go for reading a wide range of everyday materials including documents, letters, bills, menus, timetables and instructions etc. Typical features include the ability to take a snapshot of something that can subsequently be magnified, rather than having to hover with the magnifier in place. The increased adaptability of modern smartphones has, to some extent, superseded these devices (figure 5).
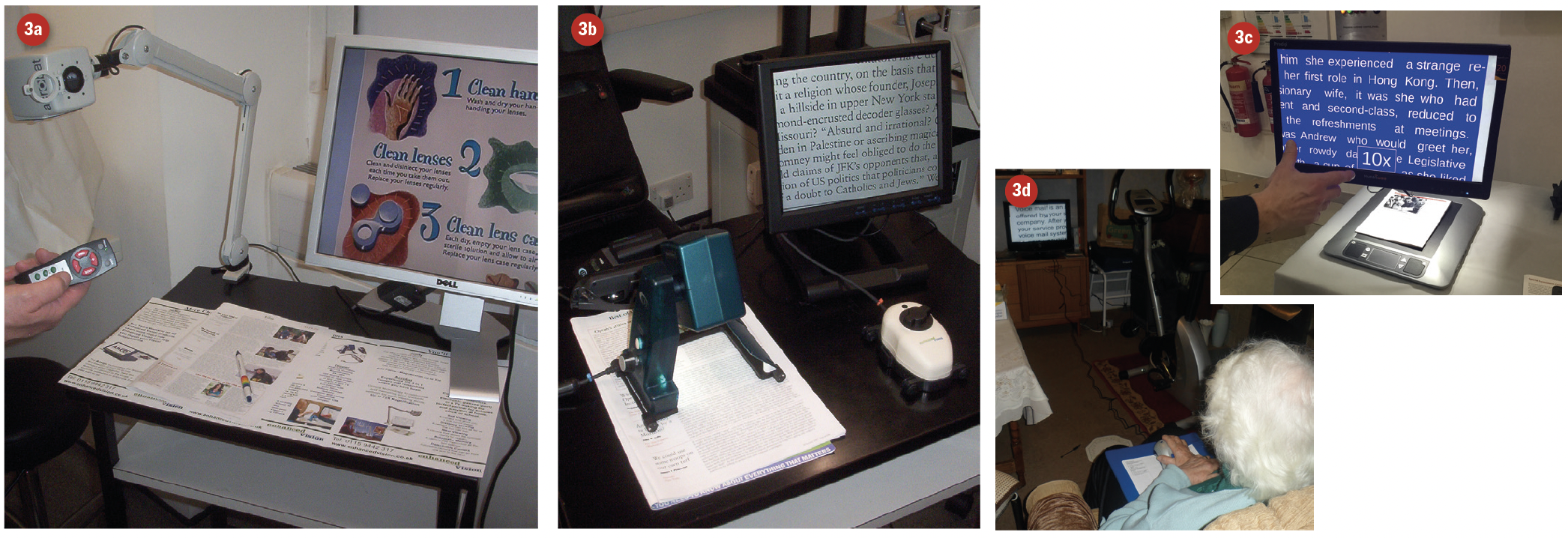 Figure 3: A selection of desktop EVES
Figure 3: A selection of desktop EVES

Figure 4: Portable EVES. 4c is focused upon a wall of the adjacent building some 10 metres away

Figure 5: Pocket EVES
The distinction between reading machines and EVES has significantly reduced in recent years, with many EVES now also including the option to hear text being read out loud.
Head-set Units
Recent years have seen a rapid growth in the number and functionality of electronic devices which are worn as head-sets in front of the user’s eyes. As such, they can display the image immediately in front of the gaze of the user but enhanced in a way that may help to overcome the user’s visual deficit. This might be by means of enhancement of the real world image using magnification, colour and contrast manipulation, by use of supporting audio description (as with the OrCam systems, figure 6) or with the use of augmentation of the input by use of virtual reality projection or repositioning of an image upon still functioning retina. Such devices work in a similar way to how Peli prisms work. An example of such a device is the OxSight Prism glasses shown in figure 7.
 Figure 6: The OrCam MyEye 2 offers audio description of a target in view
Figure 6: The OrCam MyEye 2 offers audio description of a target in view

Figure 7: OxSight Prism spectacle device
Head-set units currently available include:
- OxSight Onyx; see page 26. This unit offers a 70º field of view, 8x magnification and the ability to recognise text, faces and objects
- eSight 3; the unit offers 24x magnification with options to freeze frame capture, adjust colour and contrast, and switch between TV, reading, indoor and outdoor vision modes (figure 8)
- NuEyes; a lightweight (88g) spectacle device offering a 52º field of view with enhancement options (figure 9)
- IrisVision; a headset offering a 70º field and 14x magnification, with further functionality including OCR, image enhancement and internet linkage for streaming online video and other media (figure 10)
 Figure 8: The eSight3
Figure 8: The eSight3
 Figure 9: The NuEyes device
Figure 9: The NuEyes device
 Figure 10: IrisVision Live
Figure 10: IrisVision Live
Affordability and Challenges
Unsurprisingly, there are disadvantages to EVES. With a lack of funding, for many patients cost can be a major inhibitory factor. Though EVES are less expensive than previously was the case when first introduced, it remains a considerable outlay, especially for a device with a limited time of usefulness (as is often the case with the very elderly or those with a progressive condition). Some manufacturers allow patients to trial devices before purchasing. Some larger low vision resource centres may have devices to try ‘on site’ with staff available to aid selection and give training. In addition, some low vision clinics may also have visiting staff at specific times who will demonstrate a selection of EVES. As with any equipment of this nature, there is a risk of them developing faults that may be complicated to rectify, and as the value of the device will depreciate quickly, users may have to decide if they feel it is worthwhile paying for repair.
As with any technology, EVES will become outdated relatively quickly, though to most patients, this is not a disadvantage per se. Due to the nature of the device, a power supply is usually required, which, if mains only, may reduce portability and present a trip hazard. If battery powered, this could also be considered a disadvantage due to the costs, while changing the batteries can sometimes be a challenge in itself. Many suppliers and manufacturers have made significant improvements to facilitate an easier access to battery compartments. Readers may agree that this point applies to all illuminated low vision aids. Even though many traditional optical magnifiers may also require battery power, the battery life is frequently longer with these as compared with EVES. It could also be argued that electronic devices need more maintenance than optical ones, though this is debateable.
With the larger devices, portability may be limited anyway, though there are an increasing number of portable choices. A disadvantage with earlier portable devices was a lack of robustness and durability, with some early adopters suffering breakages and damage after just a few excursions. Robustness has improved greatly in recent years. The additional training required for optimal usage may be a hindrance to some, but it should not be forgotten that even simple hand magnifiers may require training in their correct use. The aforementioned advantage of availability of higher magnification with EVES leads to the disadvantage, as with any magnification system, of a poorer field of view. As expected, the optimal use including best reading speeds will be achieved when using minimum magnification as this will give the patient the maximum field of view. There may also be, depending again on the device, some difficulty with examining curved surfaces or objects.
Unlike traditional optical magnifiers, EVES are often not available for funding via the NHS. This is changing, however, and the Welsh Low Vision scheme, for example, offers the supply of an EVES device where its usefulness can be argued. Also, as many patients already own computers, tablets and smartphones, access to electronic magnification is often very cheap and easy.
There is statutory provision, following assessment, for those who are deemed eligible; those in full time education or those in employment via the ‘Access to Work’ scheme (throughout the UK except Northern Ireland).1
For those in education, children are ‘statemented’ and receive an education and healthcare plan (EHCP), formerly known as a statement for Special Educational Needs that outlines the help they require, which may include EVES (figure 2). The Access to Work scheme provides practical support and financial help for those with visual impairment and other disabilities. Some charities may help certain individuals, for example St Dunstan’s (Blind Veterans UK) may help those previously or indeed currently in the armed forces. If not, eligible patients will need to purchase EVES privately, with some charities (such as the Macular Society) offering limited help and possibly access to second-hand markets, which may reduce costs.
It is worth noting that adaptive technologies are eligible for VAT relief. A person may be eligible to claim VAT relief if they, or the person for whom they are purchasing, are visually impaired, blind, have another disability, or if they are buying on behalf of a charity. VAT reliefs for disabled people are not means-tested. They are not dependent on the benefits a disabled person may or may not get and a person does not have to be registered disabled in order to qualify.2
Currently, this author is trialling several assistive and adaptive options with patients, including those openly technophobic, to see how they may perform with EVES as an alternative to traditional optical devices. The key study already published in this area is the p-EVES study.3-6
The p-EVES Study
The p-EVES Study was designed to answer the question of whether p-EVES devices offer real benefits to users for near tasks and activities, in addition to traditional optical LVAs.2 The p-EVES Study was a prospective two-arm cross-over randomised controlled trial to determine the clinical effectiveness, acceptability, and cost-effectiveness of p-EVES devices compared to optical LVAs.
Overall, maximum reading speed for high contrast sentences was not significantly different between optical aids and p-EVES, although the critical print size and threshold print size which could be accessed with p-EVES were significantly smaller (p<0.001 in both cases), due to the higher magnification available. However, p-EVES were preferred for leisure reading by 70% of participants and allowed longer duration of reading (p<0.001). Although the original hypothesis was that p-EVES would be more versatile, and might replace several other devices, in fact the optical aids were used for a larger number of tasks (p<0.001) and used more frequently (p<0.001). The p-EVES is therefore an extra device in the clinician’s armoury, in that it complements rather than replaces other aids for near vision.3-5
The findings of the p-EVES Study are sufficiently positive to support a bid to commissioners of services to introduce p-EVES supply as a potential service development in NHS clinics throughout the UK, so they can meet the requirements of the Joint Strategic Needs Assessment for Eye Care and Sight Loss Services.
Conclusion
With the rapid evolution of electronic instrumentation, the options now available for those with vision loss are much better than was the case just a decade ago. It is important for all working in the low vision discipline to keep as up-to-date with these developments as possible, either through the academic press, the general media or from listening to their patients.
- Bill Harvey is a specialist optometrist at the RNIB.
References
- Guidance; Assistive technology: definition and safe use. Updated 12 February 2021 and available at; www.gov.uk/government/publications/assistive-technology-definition-and-safe-use/assistive-technology-definition-and-safe-use
- www.gov.uk/guidance/reliefs-from-vat-for-disabled-and-older-people-notice-7017#customer
- J Taylor, R Bambrick, M Dutton, R Harper, B Ryan, R Tudor-Edwards, H Waterman, C Whitaker, C Dickinson. The p-EVES study design and methodology: a randomised controlled trial to compare portable electronic vision enhancement systems (p-EVES) to optical magnifiers for near vision activities in visual impairment. Ophthalmic & Physiological Optics, 2014, 34(5), 558-572
- JJ Taylor, R Bambrick, A Brand, N Bray, M Dutton, RA Harper, Z Hoare, B Ryan, RT Edwards, H Waterman, C Dickinson. Effectiveness of portable electronic and optical magnifiers for near vision activities in low vision: a randomised crossover trial. Ophthalmic & Physiological Optics, 2017, 37(4), 370-384
- N Bray, A Brand, J Taylor, Z Hoare, C Dickinson, RT Edwards. Portable electronic vision enhancement systems in comparison with optical magnifiers for near vision activities: an economic evaluation alongside a randomized crossover trial. Acta Ophthalmologica, 2017, 95(5), e415-e423
Resources
A useful resource is, as always, the RNIB website. Go to; www.rnib.org.uk/sight-loss-advice/equality-rights-and-employment/staying-work/assistive-technology