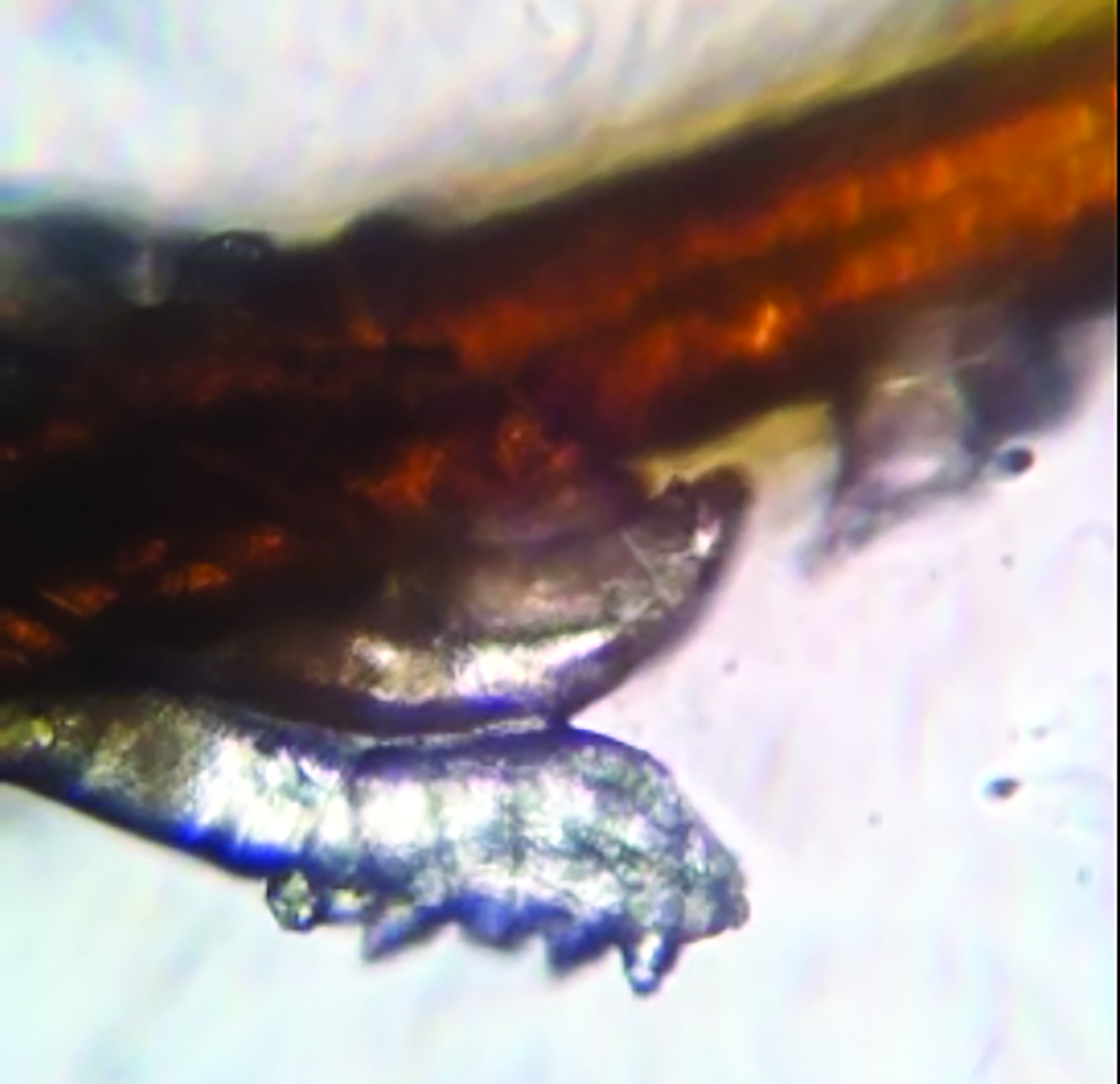
Every now and again, I find myself confronted with a light bulb moment. In professional terms, this is usually when it dawns on me that I have been completely underestimating something that I encounter regularly in clinic or with patients, but until that moment have not really spent any quality time speculating on the whys and wherefores. One such time in my career of great significance took place around 10 years ago when I first learned of the impact of Demodex spp and its influence upon the health of the ocular adnexa (figure 1). The can of worms (or mites in this case) that opened as I read that first CET article on the subject astounded me and, I can honestly say, my practice has never been the same since.
Recently, I have experienced another such lightbulb moment.
Figure 1: Demodex mite on an eyelash
Why an interest in cosmetics in eye care practice?
As an optometrist and dry eye specialist, I have long since been aware, if only on a very superficial level, of the issues with cosmetics and make-up causing irritation to existing dry eye patients (myself included) and contact lens wearers. This can result in poor tolerance or a flare-up of symptoms or both when eye make-up is applied. I have also seen numerous examples of caked layers of make-up on lids, pigment embedded in tarsal plates and floating debris in the tear films of determined wearers, enough to put you off your mid-morning chocolate chip cookie.
My general stance, until recently, was to offer standard general advice about inserting contact lenses before make-up application and ensuring all make-up was thoroughly removed at the end of each day, possibly forming part of a wider eyelid hygiene regime. In more recent years, I have also advised the use of lid hygiene products for blepharitis as a dual-purpose make-up remover. I did, however, stop short of telling patients to stop wearing make-up: that is like telling patients to stop wearing clothes. With no obvious alternative, it is definitely a non-starter. Besides which, I felt that a significant percentage of my dry eye patients were fairly self-selecting and ditched their make-up when it became too much of a burden, able to recognise when it was clearly adding to their dry eye symptoms.
Looking further into our current understanding of the issues with standard make-up, what I have learned so far has genuinely shocked me. My aim for this article, therefore, is to outline the current issues, highlight what we know, and suggest what we should be considering on a daily basis when offering advice about cosmetic use by our patients.
Firstly, why should we even consider cosmetics?
Most of us have almost certainly not given cosmetics use in our patients much thought and are unlikely to be routinely asking questions during our consultations about patient’s current periocular cosmetic habits.
A recent study,1 however, highlighted that the prevalence of dry eye disease among women who used eye cosmetics was over 70%, much higher than the 5% to 50% among the general population.2 In addition, approximately 25% of participants using eye make-up rarely removed it before sleep. This was shown to be a further significant risk factor in the severity of dry eye. Given these figures, the impact of cosmetic products is something eye care practitioners cannot afford to ignore any more.
What are cosmetics?
Cosmetics come in all forms, though they are generally considered products that are rubbed, poured, sprinkled on, and or sprayed on the body and face to ‘beautify’ oneself. The use of cosmetics, by both men and women, has been around since ancient Egyptian times. Back then, cosmetics were used for a variety of reasons; to enhance beauty, to imitate the gods, for health, to protect the skin from the sun, and even to ward off evil spirits.
Nowadays, the cosmetics that patients use on and around their eyes are not required to meet the same type of regulatory standards as ophthalmic pharmaceutical products, despite consisting of a wide range of chemicals, many of which are known not to be inert.
On average, women use 12 personal care products a day, exposing themselves to 168 chemical ingredients. Men use six, exposing themselves to 85 unique chemicals. The average age at which girls start to use cosmetics is around 12 years of age.
What ingredients are in cosmetics?
As a practitioner, we encounter many different forms of agents and ingredients that we regularly recommend or prescribe to our patients, such as contact lens care solutions and ocular lubricants. However, apart from the headline recognisable ingredients, I admit that most other constituents are a bit of mystery to me. This is yet more true for the ingredients of cosmetics. The list is usually so long, and in such small print, that it is a wonder that anyone ever bothers to read it (figure 2). The problem with this, to put it bluntly, is that they are not all safe to be used near the eyes.
Figure 2: The ingredient lists on many cosmetics are often both extensive and difficult to read

This less than satisfactory situation has been allowed to continue, despite evidence of harmful effects from some constituents, because cosmetics lack the more stringent regulation required of medicines. As a result, certain ingredients in cosmetics and anti-ageing products have been identified as belonging to the following harmful classifications:
- Carcinogens
- Endocrine disruptors
- Neurotoxins
- Reproductive toxins
Why do cosmetics irritate dry eyes?
Cosmetics and anti-ageing treatments used on and around the thin, and therefore easily penetrated, skin of the eyelids can, unfortunately, have an impact on the ocular surface. This impact may cause a number of adverse effects and may:
- Disrupt hormones
- Stress the ocular surface
- Increase the inflammation-inducing evaporative load of patients with ocular surface disease
- Irritate the cornea and conjunctiva
- Cause meibomian gland dysfunction and contribute to meibomian gland loss
- Contaminate the tear film
- Create tear film instability
- Promote demodex infestation
- Cause or exacerbate dry eye disease
Take, for example, benzalkonium chloride. This is a preservative and antimicrobial agent widely known among the eye care professionals as an ingredient that causes insult to the ocular surface.2 It is also authorised by the European Union for use in cosmetic products at maximum concentrations of 0.1% (1 mg/ml).4 This concentration is 20,000 times greater than that found to be toxic to human corneal, conjunctival and meibomian gland epithelial cells.
Other preservatives widely used in cosmetic products are formaldehyde (FA)-releasing compounds. According to Harvard Medical School research, the approved limit in cosmetics for FA-releasing compounds is some 740 to 2,000 times higher than the concentration shown to be toxic to human corneal, conjunctival and meibomian gland epithelial cells.5
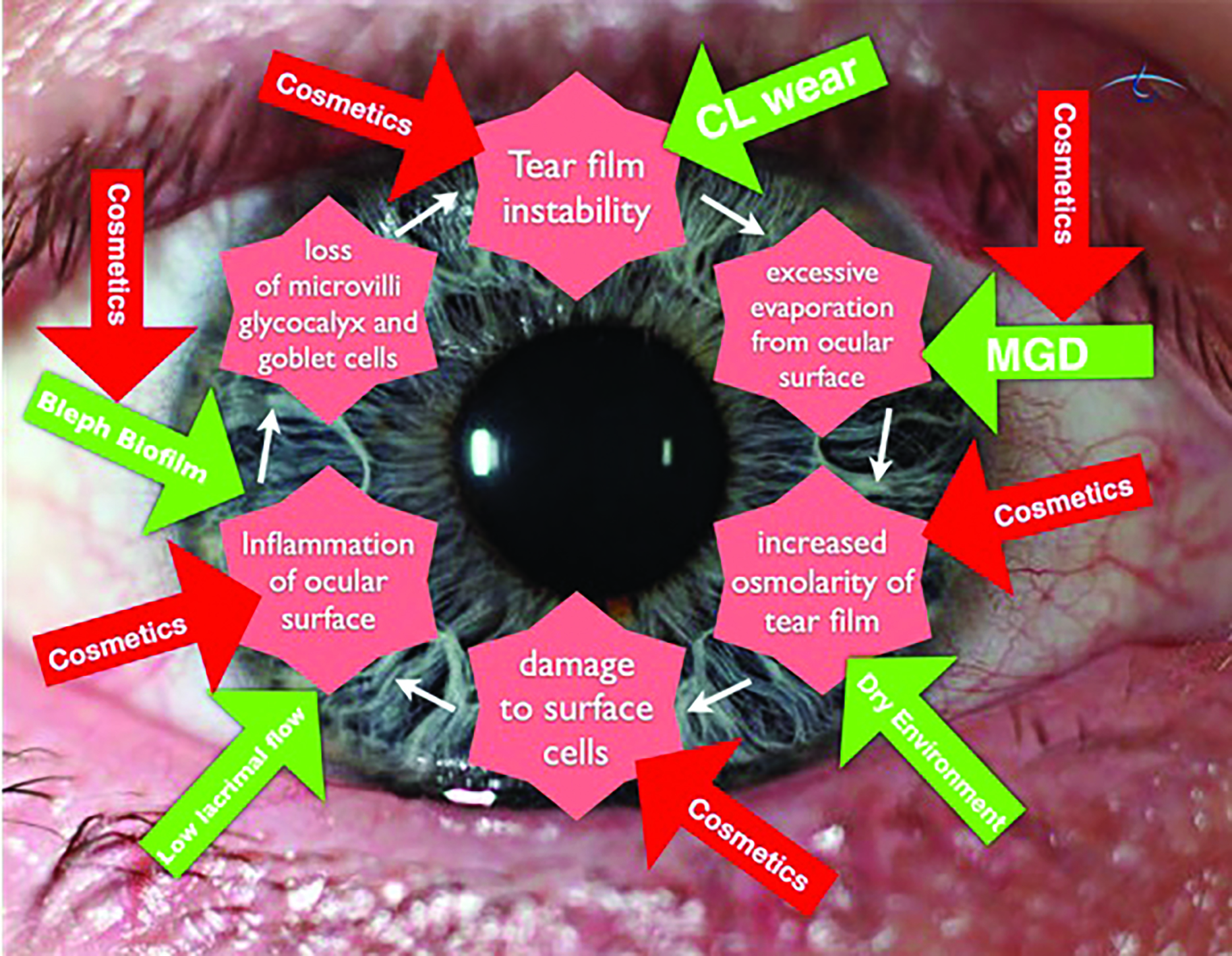
It is now accepted that dry eye disease persists and progresses as a vicious circle, one fuelled by a number of factors. Figure 3 shows various points of this circle where cosmetics can exacerbate the situation.
Figure 3: The vicious cycle of dry eye disease and the key points that can be influenced by cosmetics (red arrows)
What cosmetic ingredients should we encourage patients to avoid?
It is way beyond the scope of this article to list all the chemicals in cosmetics that might be worth avoiding, and this list is ever-growing as further research into adverse effects is undertaken. Interestingly, the US only bans 11 chemicals for use in the formulation of cosmetics, while the EU (and formerly the UK) bans more than 1,300. While this does make our job as eye care professionals rather difficult when patients ask for succinct and efficient advice, it is, at least, possible to provide information about some of the worst culprits. Table 1 lists 10 key ingredients to avoid, but remember that this is by no means an exhaustive list.
Table 1: Ten cosmetic ingredients known to cause damage to the ocular surface and adnexa
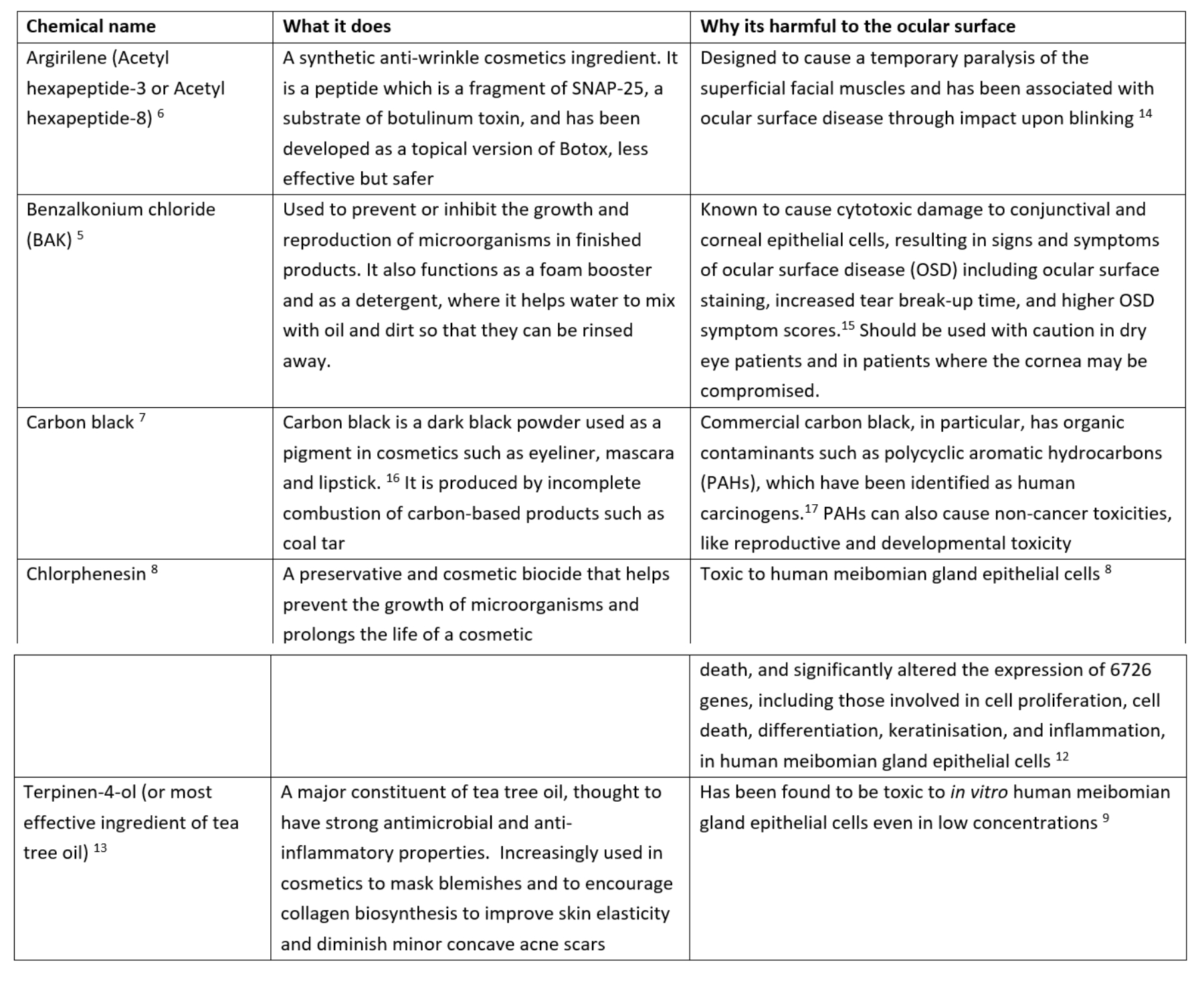
It is worth noting the inclusion of terpinen-4-ol in this list, a key ingredient in many cosmetic tea tree oil-based products. It is also found in lid cleansers specifically designed to treat Demodex blepharitis as it has proved to be effective in killing demodex mites present on lash follicles. However, the ingredient has also been shown to cause a toxic effect on meibomian gland epithelial cells in vitro.5, 13 Because of this, it is always best to look at the overall risk-to-benefit ratio for any individual with a need to control their Demodex population, as well as to consider the appropriate minimum frequency and duration of use for each patient individually.
Anti-ageing and anti-acne products
A significant number of anti-ageing products, and anti-acne creams, that are widely available in many countries contain retinol, also known as vitamin A or all-trans retinoic acid. Indeed, you may have some in your own bathroom cabinet at home. Retinol is obtained in the diet from plant or animal sources. Retinoic acid is the most active biological form of vitamin A while retinyl palmitate is the major storage form of vitamin A in the skin.
Retinol is found primarily in anti-wrinkle creams while another variant, called isotretinoin (13-cis-retinoic acid), is sold as Roaccutane; a common anti-acne cream. Retinoic acid is known to have a direct and significant damaging effect on meibomian glands.12 Indeed, it is not uncommon in my dry eye clinic to see younger patients who have been on isotretinoin to have significant gland loss at very young ages.
Bad Habits
When we consider our own daily lives, most of us have many bad habits, perhaps more than we would ever want to admit in public, usually stemming from lack of time, ignorance or simply laziness. This is evident on a daily basis in my dry eye clinic, where patients frequently confess to practices that make my toes curl.
There are a number of typical bad habits to look out for regarding eye make-up use. These include:
- Sleeping in eye make-up
- Sharing eye make-up
- Not replacing eye make-up regularly; mascara tubes can harbour a multiplicity of pathogens (figure 4). Many women keep their mascara for six to 12 months or more and, worse still, have been known to spit in the tube or add tap water to prolong use of the product.
- Waterline (the inner eyelid margin) application of eyeliner
Figure 4: Mascara tubes can harbour a multiplicity of pathogens

The term waterline is not a medical, anatomical label but a description coined by the fashion industry to describe the gap posterior to the eyelashes to the mucocutaneous junction along the lid margin at the point where the tears end and where the meibomian gland openings are to be found. Despite centuries of well-meaning advice to avoid using eyeliner along this zone, many wearers still persist in applying liner onto this area for some perceived improved cosmetic effect, whether real or otherwise. The concern about doing so hinges upon the potential for cosmetic product to enter the tears and onto the ocular surface to cause an adverse response.
A small but elegant study to verify the truth behind the risk of using eyeliner on the waterline was carried out by researchers from Cardiff and Waterloo Universities.19 The aim was to compare how much material from a conventional pencil eyeliner, applied to the periocular skin along one of two different locations, would subsequently migrate and contaminate the tear film. The two locations chosen were the waterline, the space behind the lash line, and the periorbital skin immediately anterior to the lash line (figure 5). The level of contamination was assessed by counting the number of glitter particles seen in the tears on slit lamp examination.
Figure 5: (a) Eyeliner applied anterior to the lash line. (b) The so-called waterline, as delineated by the red marker. Note that, several days after removal of eyeliner, particles of cosmetic can still be seen in this region
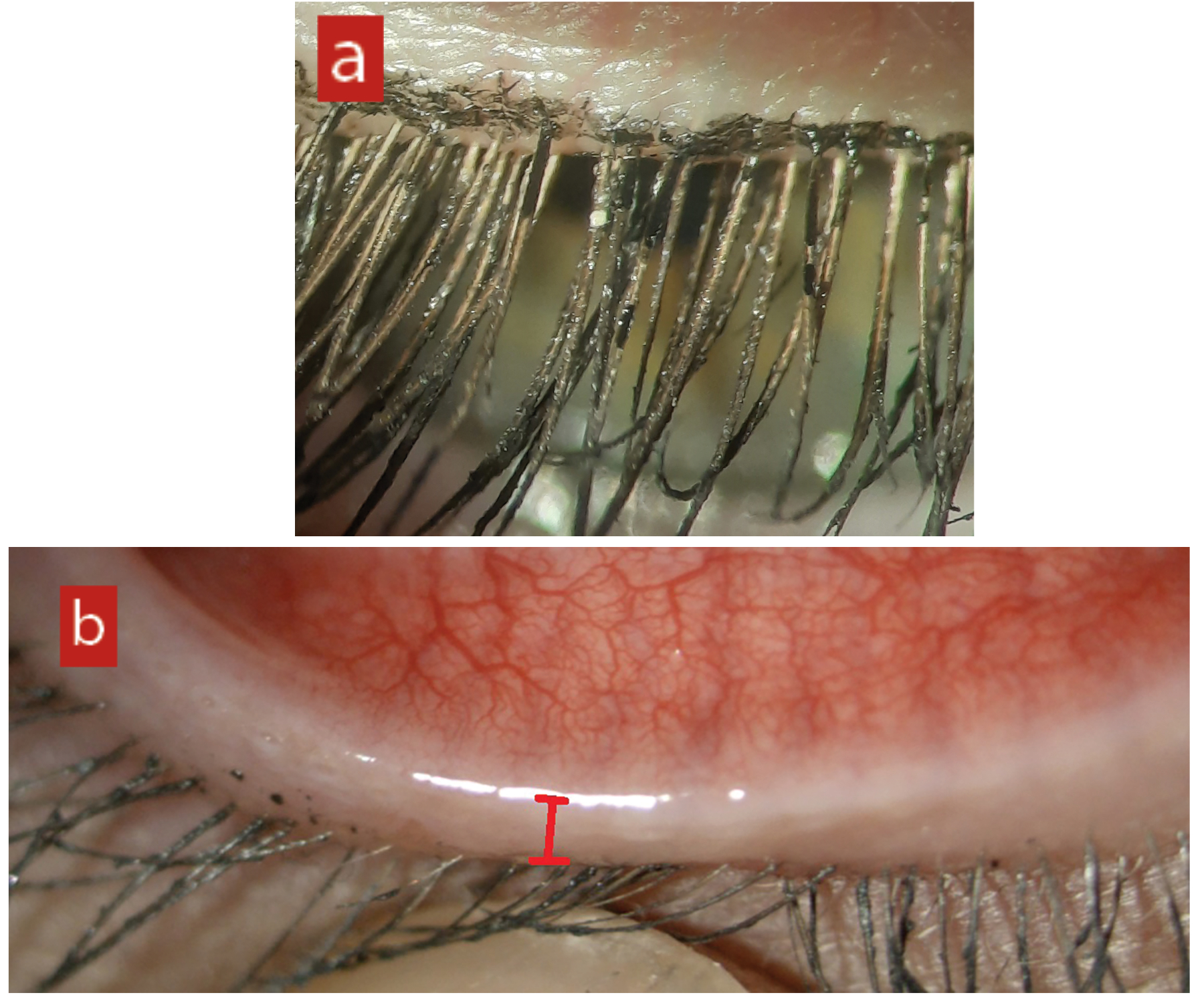
The results clearly supported the view that ‘eyeliner migrates most readily and maximally contaminates the tear film when applied posterior to the lash line.’ The study concluded that ‘it would be beneficial to advise patients to reserve the application of eyeliner pencils to anterior to the lash line… People who wear contact lenses are most likely to notice some problems. If they have eyeliner stuck to their lenses, increasing deposits might cause vision disruption as the lens becomes cloudier.’
It is worth directly addressing these common make-up misdemeanours. This can serve as a good starting point in encouraging your patients to adopt better cosmetic health practice.
Starting the conversation about make-up with your patients
Most practitioners do not have time to chat with patients. Nor do they have the specialised background in biochemistry that would be needed to analyse all the listed ingredients in any cosmetic product. Sometimes, instead, the easiest way is to infuse some humour into the conversation about hygiene practices. For example:
- ‘Do you remove eye make-up before going to bed, or wake up with panda eyes in the morning?’
- ‘Waterline eyeliner or mascara is like water-boarding the meibomian glands.’
- ‘How often do you replace your mascara? Remember, bugs are having sex on your eyelashes.’
Admittedly, I will tend to only scratch the surface of this topic in a normal eye examination at best. But, during my dedicated dry eye work ups, a ‘current cosmetics review’ is now an essential part of my routine battery of baseline questions and assessments.
Contact Lens Wear and Cosmetics
There is obviously a significant number of contact lens wearers who also wear make-up. Often the two modalities go hand-in-hand as there is a beauty enhancing element given over to both sides of this equation. As practitioners, we need to be aware that introducing make-up to a contact lens-wearing eye also carries with it some risk.
Mascara and microplastics, such as the glitter in eyeshadow, can be both mechanically and chemically irritating if they flake into the tear film. These flakes can become trapped under soft or rigid corneal contact lenses. Pigments used in eye make-up might not be water-soluble and so can become lodged under a lens and potentially damage the ocular surface or cause corneal abrasions.20
Are Permanent Cosmetic Enhancements Better Than Daily Cosmetic Products?
A not uncommon question from patients in my dry eye clinic is whether it is better to use more permanent or semi-permanent solutions instead of daily make-up. Such treatments include eyelash tinting, eyelash extensions or growth serums. The recent obsession on social media for extra-long lashes does not help in this regard.
False Lashes
Sadly, this is another area of concern when it comes to ocular surface health. The adhesives used are cyanoacrylates, which adhere the false lash to the existing lash and often contain volatile organic compounds and preservatives, such as formaldehyde. Upon application, these chemicals can enter the eye and induce chemical conjunctivitis or keratitis. During wear, these products have been associated with contact dermatitis, allergic reactions and inflammation, which may also exacerbate existing blepharitis.
The other issue with false lashes is that patients may avoid proper lid cleaning for fear of dislodging the extensions. This also adds to the ideal conditions for all manner of micro-organisms to establish.
Eyelash Tinting
Lash tinting is associated with severe conjunctival reactions and acute inflammation due to chemical toxicity as well as allergic response.
What should we be recommending?
As well as advising patients what to avoid, we really need to consider what products to recommend. Just as in other areas of my dry eye practice, I stock a range of products that I want individuals to actually use. Compliance is better when a product is readily available and easy to start using. I prescribe a range of unique ocular surface-friendly make-up products known as ‘Eyes Are the Story’ (see case study on page 30 or go to eyesarethestory.com for more information). I also explain detailed application and removal techniques, just as I prescribe lid hygiene and lubricants, as part of a comprehensive tailored plan for each patient I treat.
A complex problem with a complex answer?
As part of the wider picture of tackling dry eye disease in our patients, and let us face it that task alone is challenging enough, we must now add cosmetics to our ever-expanding list of considerations regarding eye health.
Personally, my journey to understanding the cosmetic challenges associated with dry eye has, so far, only enhanced my ability as a practitioner to further advise and help those patients attending my dry eye clinic with appropriate clinical evidence based advice. Any revision to my dry eye practice simply serves as a reminder that we can never stand still as practitioners. Embracing the latest research and ideas really does translate directly into healthier and happier patients.
The Future
The highly anticipated next TFOS report, entitled A Lifestyle Epidemic, will be published in the near future (figure 6). This will, no doubt, look at the wider context of modern lifestyle and what can drive the exacerbation of what we know as dry eye disease.
Figure 6 & 7 (left to right): Still from a launch video from TFOS announcing forthcoming plans to publish the latest report, A Lifetime Epidemic. The impact of cosmetics will be included in the review; and Heavily applied eyeliner can easily mask underlying blepharitis
My Top 10 Cosmetic Clinical Considerations
- Be realistic; patients who currently wear any forms of eye make-up are unlikely to want to give it up completely.
- Advise patients to remove all make up at the end of the day with a good lid hygiene product (such as those to treat blepharitis).
- Be aware; eyeliner, mascara or eyeshadow can mask or mimic blepharitis (figure 7). Take a careful look during your consultation and do not be afraid to ask the patient to remove their eye make-up for a better look if necessary.
- Do not forget the men’s beauty market has grown significantly in recent times.
- Good patient education is paramount.
- Labels such as ‘plant-based’, ‘natural’, ‘organic’, ‘vegan’ and ‘ophthalmologist-tested’ do not equate to ocular surface safety.
- Be extra aware of the implications of cosmetics for contact lens wearers.
- Consider enhanced antimicrobial management in cosmetics users with advice on daily hypochlorous acid sprays onto the lids and periorbital skin.
- Alternatives to daily cosmetics, such as false lashes, also put the ocular surface at risk.
- Consider recommending or even stocking dry eye friendly cosmetics (such as the ‘Eyes Are The Story’ opto-cosmetic range).
- Sarah Farrant is a therapeutic optometrist with a specialist interest in dry eye disease and myopia management practising in Somerset, UK.
References
- Albdaya NA et al. Prevalence of dry eye disease and its association with the frequent usage of eye cosmetics among women. Cureus, 2022;14(7):e27142.
- Gomes JAP et al. TFOS DEWS II: Iatrogenic report. The Ocular Surface, 2017, Volume 15, Issue 3, pps 511-538
- https://www.ewg.org/personal-care-products-safety-act-would-improve-cosmetics-safety (Accessed 12/09/2022)
- Regulation (EC) No 1223/2009 of the European Parliament and of the Council of 30 November 2009 on cosmetic products (recast)
- Chen X et al. Toxicity of cosmetic preservatives on human ocular surface and adnexal cells. Experimental Eye Research, 2018; 170: 188-19
- Ozgur O et al. Dry eye syndrome due to botulinum toxin type-A injection: guideline for prevention. Hawaiian Journal of Medicine and Public Health, 2012; 71(5): 120-1237
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Carbon black evaluation and rationale. 2010; 93: 43-190
- Wang J et al. Toxicity of the cosmetic preservatives parabens, phenoxyethanol and chlorphenesin on human meibomian gland epithelial cells. Experimental Eye Research, 2020; 196:108057
- https://www.cosmeticsandtoiletries.com/regulatory/claims/120476614.html (Accessed 8/9/22)
- Horváth O et al. Periocular discoloration after using a prostaglandin analog for eyelash enhancement: evaluation with reflectance confocal microscopy. Journal of Cosmetic Dermatology, 2017; 16(1): 18-20
- Kam WR et al. Do cyclosporine A, an IL-1 receptor antagonist, uridine triphosphate, rebamipide or bimatoprost regulate human meibomian gland epithelial cells? Investigative Ophthalmology and Vision Science, 2016; 57: 4287-4294
- Ding J et al. The influence of 13-cis retinoic acid on human meibomian gland epithelial cells. Investigative Ophthalmology and Vision Science, 2013; 54: 4341-4350
- Chen D et al. Effects of terpinen-4-ol on meibomian gland epithelial cells in vitro. Cornea, 2020; 39: 1541-1546
- Sonali T et al. Complications and adverse effects of periocular aesthetic treatments. Surveys in Ophthalmology, 2022, Vol 67, Issue 3, p741-757
- Goldstein MH et al. Ocular benzalkonium chloride exposure: problems and solutions. Eye, 2022, 36, 361–368
- International Carbon Black Association. Available online: http://www.carbon-black.org (Accessed 26/4/2022)
- National Toxicology Program. Report on Carcinogens, Twelfth Edition. Polycyclic Aromatic Hydrocarbons. Available online: https://pubmed.ncbi.nlm.nih.gov/21822324 (Accessed 26/4/2022)
- Lv C et al. Investigation on formaldehyde release from preservatives in cosmetics. International Journal of Cosmetic Science. 2015,37(5):474-8
- Ng, A et al. Migration of cosmetic products into the tear film. Eye & Contact Lens: Science & Clinical Practice, 2015, Vol 41, Issue 5, p 304-309
- Uematsu M et al. Corneal erosion with pigments derived from a cosmetic contact lens: a case report. Eye and Contact Lenses, 2018; 44(Suppl 1): S322-S325