It is hard to imagine that by the year 2050, 50% of the world’s population could be myopic.1 Yet, that is the prediction. The associated prediction that 10% of the population will have high myopia puts pressure on the eye care industry to act now to intervene to avoid this becoming a reality.1
Eye care professionals (ECPs) now have access to methods that can slow down the progression of myopia. These include MiSight 1 day contact lenses, which have been shown to slow down the rate of progression in a group of children who were aged eight to 12 years at time of initial treatment when compared with children wearing a standard single vision contact lens.2
This article will summarise what has been learned over the seven years of the MiSight 1 day clinical study. The results from the study help provide answers to some of the key questions in myopia control. This is the MiSight 1 day clinical story.
Where does the evidence come from?
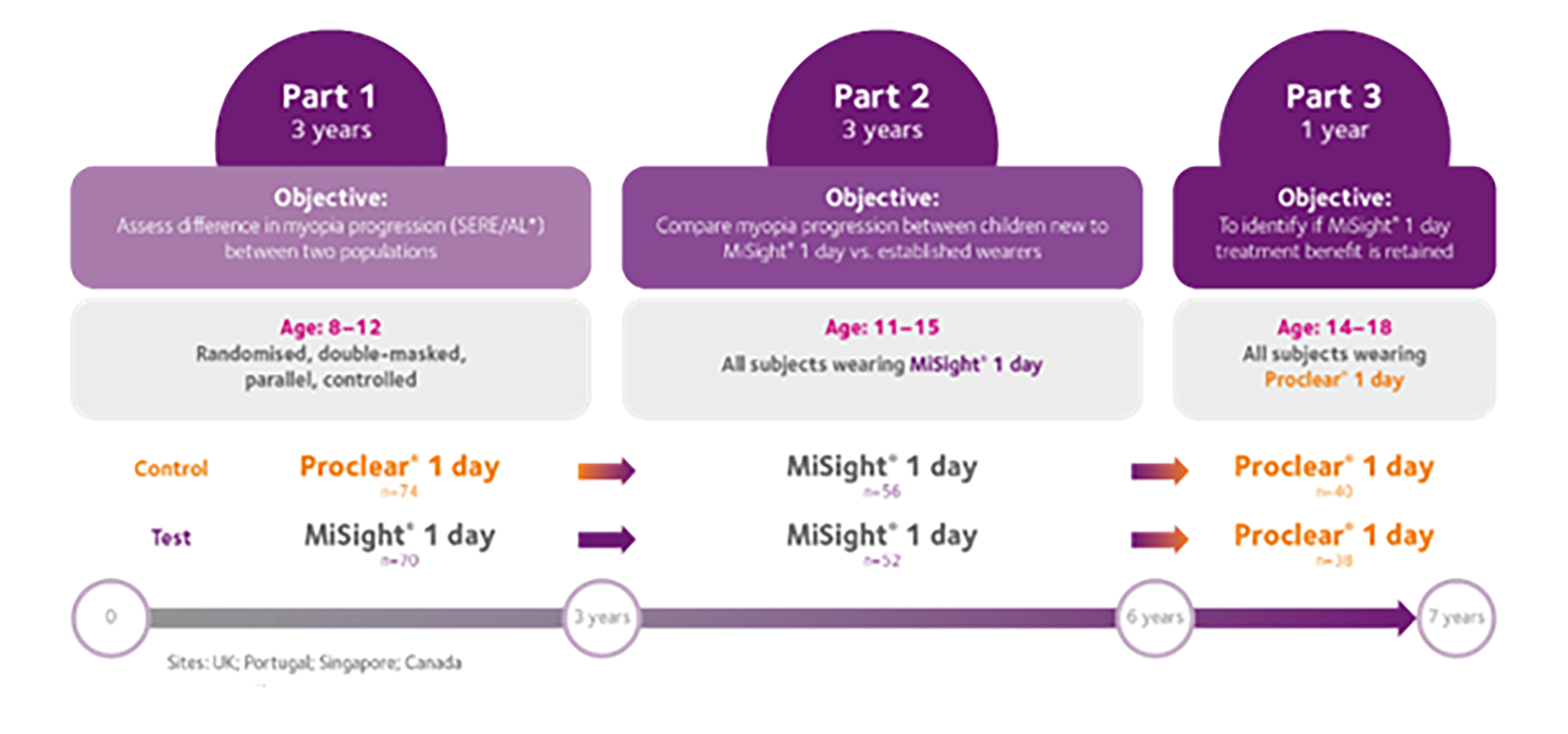
The MiSight 1 day clinical study is the longest running soft contact lens study for children at the time of writing. Four clinical sites across four countries (UK, Portugal, Canada and Singapore) were involved in the initial three years of the study, which followed a classic randomised clinical trial model, with half of the children wearing dual focus, myopia control MiSight 1 day and half wearing the single vision control lens (Proclear 1 day). At the end of the initial three years, it was evident that there was a significant difference in rates of myopia progression between the two groups. From an ethical perspective and to help maintain retention rates, children were offered the option to remain in the study for another three years with those who had been assigned to Proclear 1 day now wearing MiSight 1 day. This meant that, from the beginning of year four, there was no control group.
This extension to the study resulted in some children with six years of experience in MiSight 1 day contact lenses, and others coming into MiSight 1 day contact lenses three years after the study began, having worn standard single vision contact lenses for three years. After six full years all children were given the option to be evaluated for one more year in order to assess whether the treatment benefits of MiSight 1 day were retained once the treatment was stopped. Consequently, this final year saw all the children ceasing MiSight 1 day lens wear and moving into single vision Proclear 1 day contact lenses.3 Figure 1 illustrates the seven-year study timeline.
Figure 1: MiSight 1 day clinical study seven-year timeline.3-5 *Populations based in UK, Portugal, Singapore and Canada.
SERE= spherical equivalent refractive error. AL=axial length
The results from the initial part 1 (three years total) and the subsequent part 2 (six years total) of the study have been published in an open-access format and can be referred to for a more in-depth analysis.3, 4
Will MiSight 1 day work for all myopic children?
MiSight 1 day works for nearly all children with myopia.3
Traditional clinical trial analysis reports on the cohort mean, which for MiSight 1 day reveals a 52% and 59% reduction in axial elongation and refractive error respectively.4
Average eye growth also slows to levels seen in young emmetropic eyes.6 However, this traditional clinical trial analysis approach fails to reveal if some individuals respond better to treatment than others, or if some eyes respond while others receive no treatment benefit. The most recent analysis of those individual eyes that transitioned from the control to the treatment lens showed that MiSight 1 day works by slowing the rate of myopia progression for 90% of children.3 This means ECPs can confidently prescribe their patients with MiSight 1 day knowing that almost all will be benefitting from treatment. Most will not need a stronger prescription by their next annual eye examination, which means children will be able to see well between clinic visits, helping them at school and other aspects of their lives.2, 6 One of the most significant findings showed the greatest slowing of eye growth and myopia progression in those faster growing eyes, and this effect reflects the reported ‘proportional slowing’ created by MiSight 1 day treatment. Both of these key findings are depicted in figure 2.
Figure 2: Axial growth of children in Proclear 1 day over the first three years (uncontrolled myopic eye growth) is plotted along the x-axis with the growth those same children experienced in the following three years when they were refitted with MiSight 1 day along the y-axis. Redrawn from Chamberlain et al, 2022.3 Points 1, 2 and 4 in the figure convey the potential outcomes
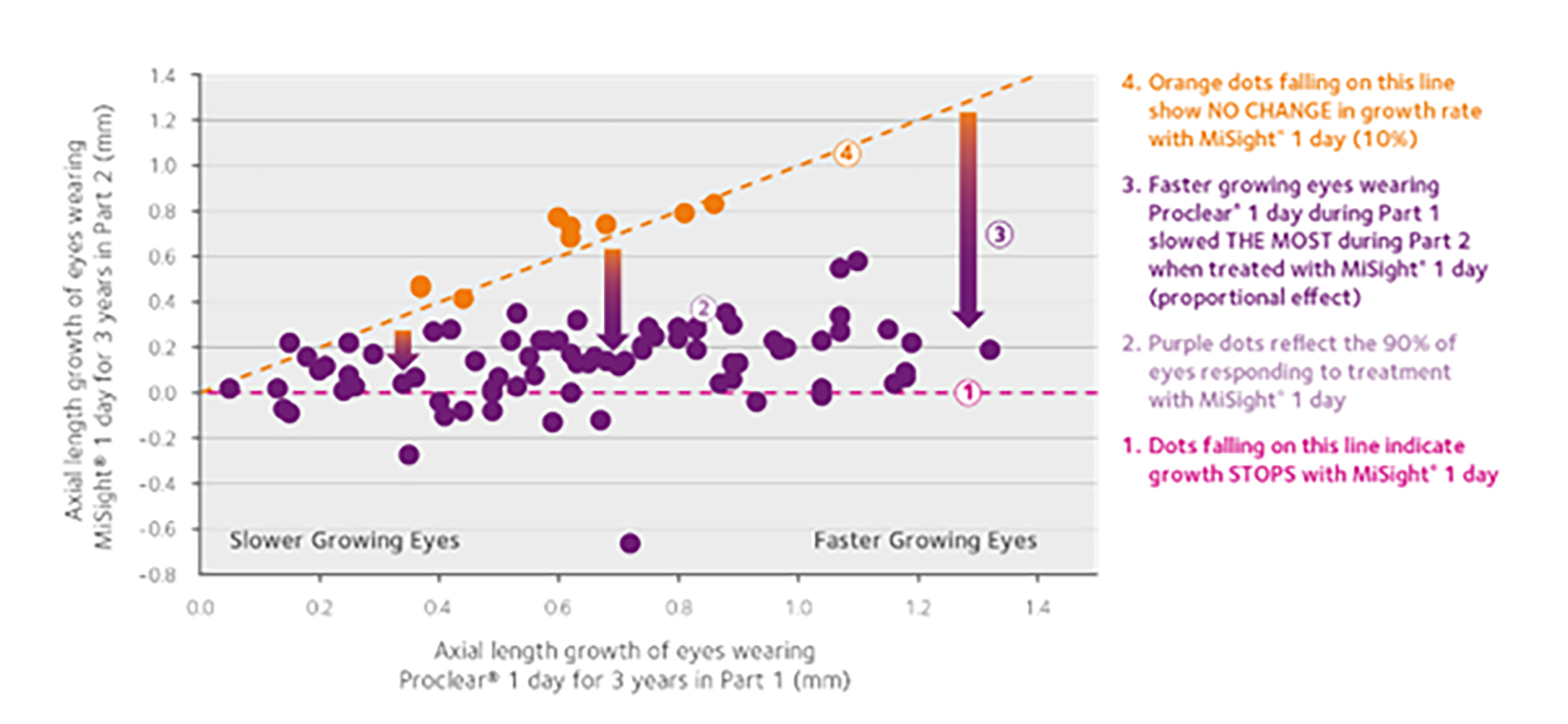
What about the 10% that did not respond? Well, first of all, this accounted for just nine eyes, which meant that the sample size was too small to provide any meaningful analysis so we are still unable to predict who will not respond to the treatment, but the powerful statistic of 90% of eyes showing a slower rate of growth (compared to the control group)3 helps provide ECPs the confidence to utilise this lens for their myopic patients.
How effective is MiSight 1 day?
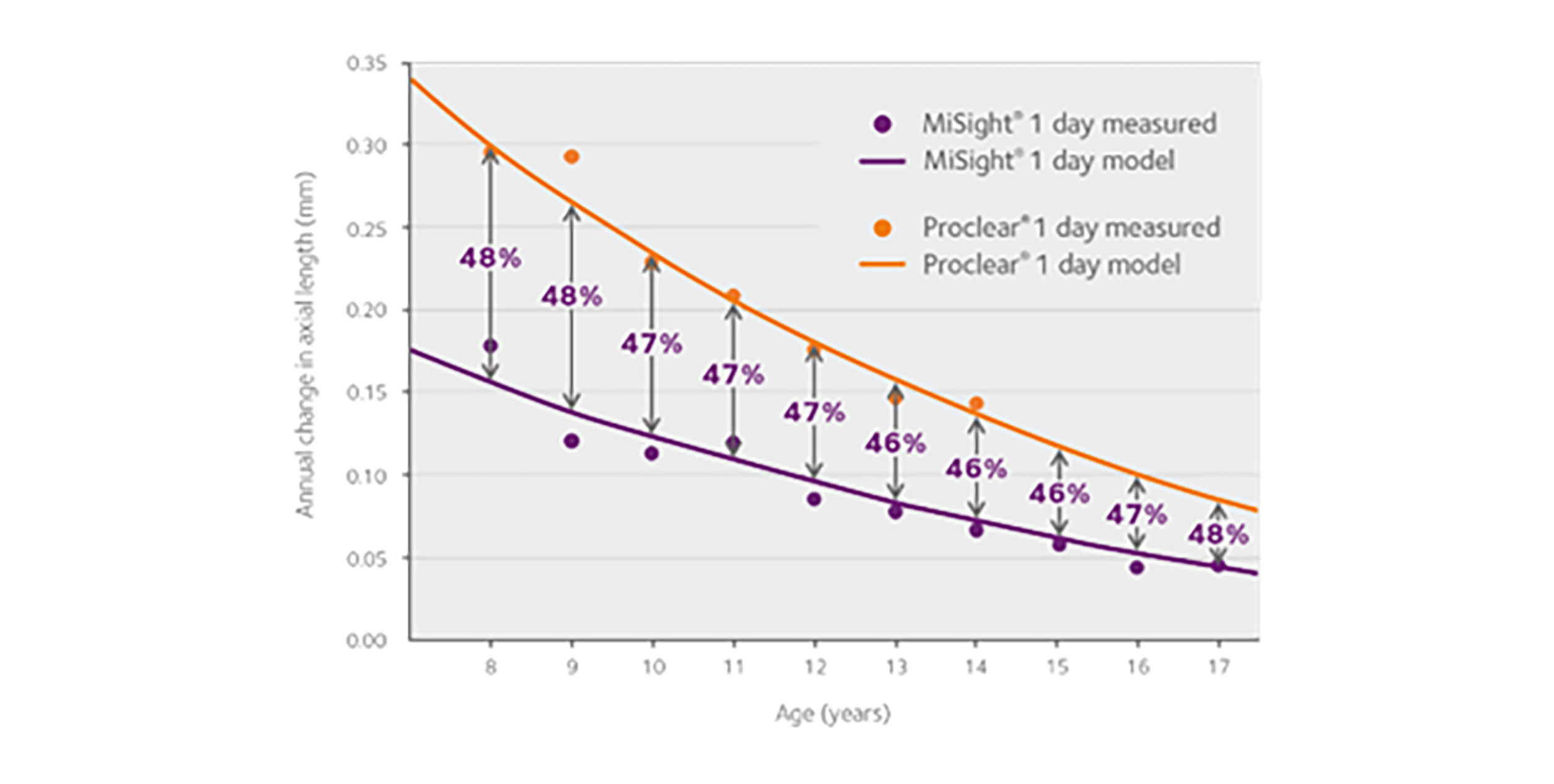
At all observed ages (8-17), MiSight 1 day slows the rate of progression of myopia by approximately 50%.7
MiSight 1 day slows both the rate of myopia progression and rate of axial elongation compared with wearing a single vision correction.2 It is essential that a myopia control intervention has an impact on both refractive error and axial elongation since eye elongation is the root cause of the myopia-associated retinal pathology later in life.8 When comparing eye growth of the treated eyes to the control eyes during those first three years, the cohort mean showed approximately 50% slower growth in the treated eyes. This approximately 50% slowing is seen at all of the tested ages (eight to 18 years),3 as shown in figure 3 where observed growth is compared to a best fit model of expected growth of untreated eyes. This result emphasises the impact of MiSight 1 day over a large number of years, thus demonstrating the benefit of wearing MiSight 1 day throughout childhood, ensuring the maximum impact on slowing the myopia progression during those years where progression is often fastest. Younger children fall on the steepest part of the progression curves, which flatten over time as children’s myopia progression naturally slows as they get older. The difference in rate remains approximately 50% between both groups regardless of age.
Figure 3: Annualized changes in axial length as a function of subject age at the start of the year over which growth was measured demonstrate MiSight 1 day slows myopia progression by half7
When to start treatment with MiSight 1 day?
Treatment should be started as soon as possible for maximum benefit but it is never too late to start.7
Children who develop myopia before nine years of age, typically have a faster progression rate than if myopia develops at an older age.9 Research also shows that the fastest rate of progression occurs in the first few months/years following the onset of myopia, and the younger the child is when they develop myopia the more likely they are to be a high myope by late teens/early adulthood.9, 10 Therefore, the message is that treatment should start as soon as possible for maximum benefit,3 although some parents and ECPs may be hesitant to start treatment, preferring to wait until there is evidence of progression.7 This is not in the best interests of the myopic child.
The evidence base is clear; ECPs should be initiating myopia control as soon as there is evidence of a myopic refractive error.
Those children who were switched from the single vision Proclear 1 day contact lens to MiSight 1 day at the 36-month mark were slightly older (11 to 15 years) and, after three years without treatment, were more myopic than the group wearing MiSight 1 day in those first three years. Eye growth in these two groups, one experiencing the first three years of treatment and the other their fourth through sixth year of treatment were the same. From this, we can extrapolate two findings:7
- MiSight 1 day treatment can be sustained over six years3
- MiSight 1 day treatment is effective when initiated after three years without treatment11
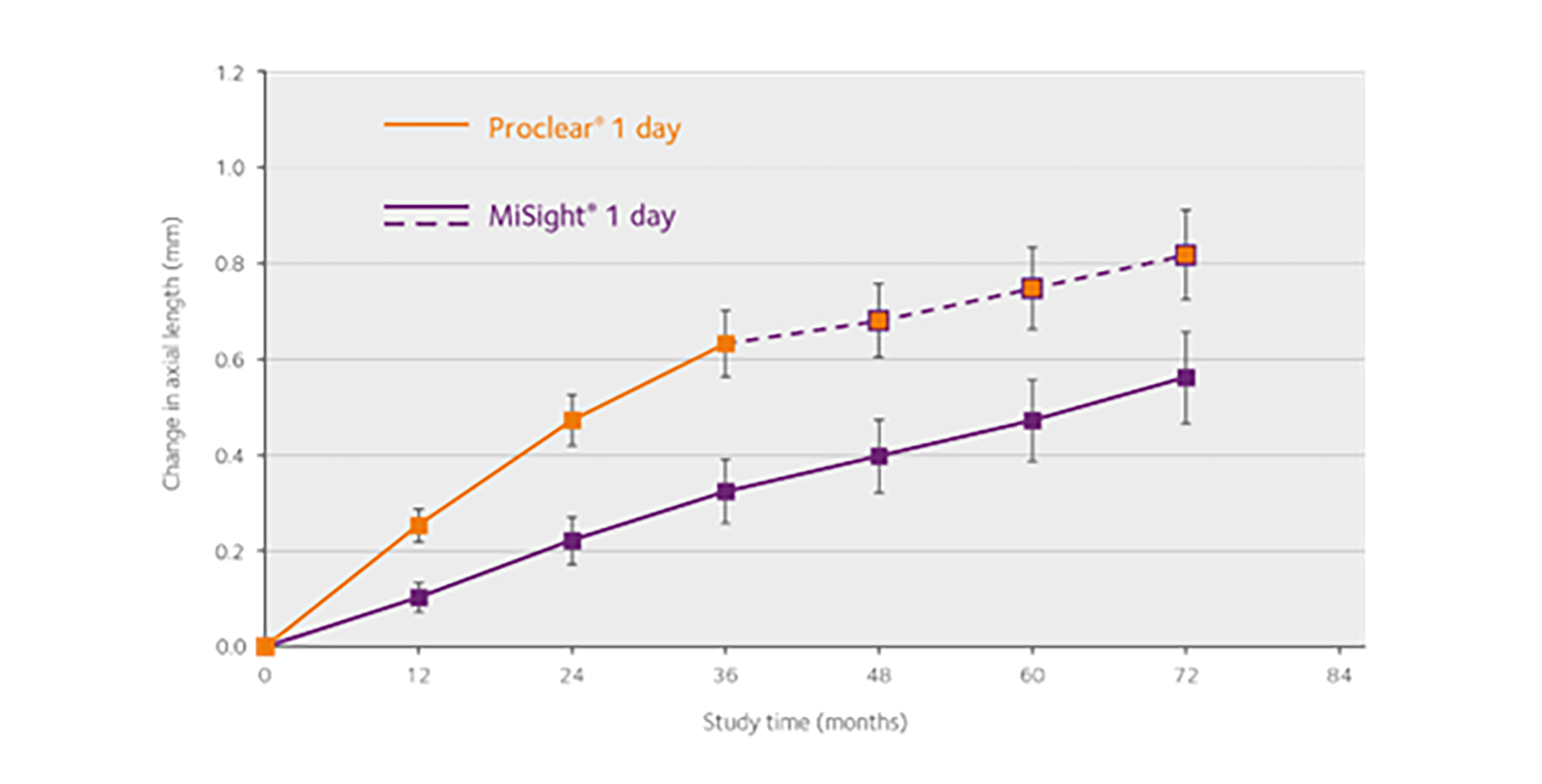
Figures 3 and 4 illustrate these points well and show that older teenagers are still likely to slow by around half. It is evident that it is never too late to start myopia control with MiSight 1 day for a patient with progressing myopia.7
Figure 4: Change in axial length throughout the MiSight 1 day clinical trial showing consistency in myopia progression rates over time while in treatment3
Is the effect of wearing MiSight 1 day sustained over a number of years?
The myopia control effect of MiSight 1 day was sustained over the period of the study.7
Some studies have shown great promise in the first year of treatment and failed to show effectiveness over multiple years.12, 13 Such a short-lived treatment effect offers little value to a child who will likely experience abnormal eye growth over many years. A truly effective myopia control treatment must exhibit sustained slowing of axial growth over multiple years of treatment. MiSight 1 day, being the longest running clinical trial of a soft myopia control contact lens, is the only intervention that can make such a claim. As shown in figure 4, the slowed growth of the treated eyes is sustained over the full six years of the treatment period (solid purple line). This plot also reveals the slowed growth in years four to six of the original untreated control group (dashed purple line), emphasising that treatment with MiSight 1 day is valuable even when initiated later in already progressed eyes.
The sustained treatment effect over six years emphasises that early concerns about a one year ‘burst effect’ for myopia control treatment do not apply to MiSight 1 day.11
Modelling the data from the clinical trial predicts the cumulative MiSight 1 day treatment effect to be at least 2.00DS (refractive error) or 0.87mm (axial length) after 10 years of wear.14 While others have suggested a ceiling effect of myopia control of around 1.00 DS to 1.50DS,15 this finding from the six-year MiSight 1 day study uses real data to model cumulative treatment and shows that long term treatment with MiSight 1 day provides ongoing cumulative benefit during the whole treatment period.7
Combining vision correction with myopia control
Can MiSight 1 day provide high quality vision while simultaneously slowing myopia progression?
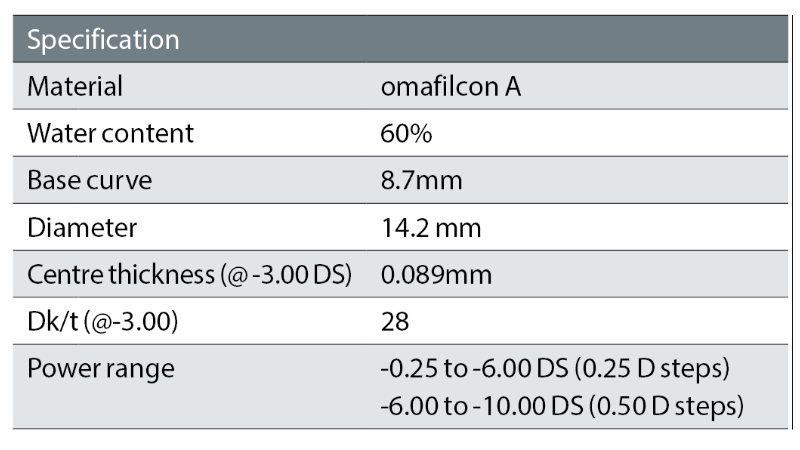
Unlike some strategies used for myopia control, such as the use of atropine drops, MiSight 1 day is available in a wide range of sphere powers (table 1) and includes a combination of myopia correction optics and myopia control optics, capable of delivering 6/6 or better visual acuity while slowing myopia progression.3 For the clinical study, all children were required to wear the lenses for at least 10 hours a day, six days a week. At the six month point in the study, the average wearing time was approximately 13 hours a day, increasing to 14 hours a day by the end of the six years,3 likely reflecting changing lifestyles as the children got older. Compliance with the wearing schedule should be confirmed at every visit and should be the first consideration if progression of myopia is more than expected.
Table 1: MiSight 1 day product specifications
How many years should a child be wearing MiSight 1 day lenses?
Myopia control should not be stopped until there is confidence that myopia is stable.
The COMET study showed that the mean age of myopia stabilisation was 15.5 years, with 48% of the children having stable myopia by 15 years of age and 77% stable by 18 years of age.15 Therefore, at 15 years of age, half of those with myopia are still progressing. There is now evidence from research to show that if MiSight 1 day is stopped, the rate of axial elongation returns to the level seen in myopes of the same age wearing a single vision correction.5, 16
It is important to consider the reasons for stopping an intervention. These could include financial reasons, problems with compliance or lifestyle changes. Where there are compliance issues, re-education of the importance of wear time to gain optimum effect may be required. When refractive error and axial elongation appear to be stable over at least two clinical visits, consideration could be made to cease myopia control. This needs to be done on an individual basis, as a teenager approaching higher levels of myopia stands to benefit more from ongoing myopia control compared to a teenager with lower levels of myopia. Careful monitoring is required with clear management of expectations that, should myopia worsen, the patient should recommence myopia control.
What happens when we stop treatment?
The benefit gained is not lost once patients stop wearing MiSight 1 day contact lenses.5, 17
It is crucial to show that the accrued benefits from treatment are retained once treatment is terminated since the value accrued from multiple years of myopia control treatment may help to reduce the risk of retinal pathology.18 Children stopped wearing MiSight 1 day at the end of year six and wore a single vision soft contact lens instead for a one-year period.5 The rate of both axial elongation and myopia progression mirrored expectations in a similar age group of myopic children not in a myopia control intervention. There is also evidence from other studies with MiSight 1 day showing similar findings.16 Therefore, this demonstrates that the myopia control effect gained over many years of wearing MiSight 1 day does not disappear when children are ready to change to a different vision correction. The benefit gained is not lost once patients stop wearing MiSight 1 day contact lenses.
Are children happy wearing contact lenses?
Ninety percent of children in the clinical study reported they were happy wearing their lenses and successful in handling them.19
It was evident from the study that the children enjoyed wearing the contact lenses with almost nine out of 10 children expressing a strong preference for MiSight 1 day over their spectacles.4, 19 This supported other work demonstrating that children enjoy and can successfully wear contact lenses.21, 22 It has been shown that children have an improved perception relating to aspects of their lives, such as participation in sports and their own appearance, when wearing contact lenses compared to spectacles.22 The excellent retention rate of 81% across the initial three years of the study and 85% across the three years of part two of the study also suggest this.3
Many ECPs and parents may be concerned about young children handling contact lenses. Parents can assist children with application of the contact lenses initially as long as the children can remove them independently. The clinical study found that, by one month, children were applying and removing their own contact lenses without additional support.19
Do eyes remain healthy when MiSight 1 day lenses are worn for six years?
Ninety-nine percent of the slit lamp findings study were grade 1 or less.22
As with all clinical studies, it was imperative to monitor for adverse events, whether symptomatic or asymptomatic. Across all of the study sites, amassing over 26,000 slit lamp observations and the equivalent of 653 years of contact lens wear, 99% of the slit lamp findings were grade 1 or less.24 There were only five instances of a slit-lamp finding greater than grade 2.22 There were no instances of microbial keratitis; the one serious event that was recorded was not contact lens-related but a uveitis secondary to Herpes zoster keratitis. These findings were in line with other studies looking at rates of contact lens complications among children and adults.23 ECPs can be confident that children wearing MiSight 1 day in accordance with the manufacturer’s instructions are at no greater risk of adverse events compared with a soft contact lens wearing adult population.4, 22
Managing expectations up front
The findings from the six-year MiSight 1 day clinical study give a wealth of information on the longer term use of MiSight 1 day to support decision-making in clinical practice. The results demonstrated are:
- The impact on myopia progression, with 90% of eyes benefitting
- The added value of treatment to fast progressors
- The excellent safety profile of soft, one-day contact lenses in children
- The positive impact for both children and parents on wearing these contact lenses.
These factors need to be considered alongside the discussion between ECPs, parents and children about the expectations:
- Some eye growth is normal, even when wearing MiSight 1 day
- It is not yet possible to predict how an individual child will respond nor guarantee final outcomes
- It is possible to be confident that the majority of children will see a benefit from MiSight 1 day treatment
- It is important to remember that children benefit from contact lens wear beyond myopia control effects and wearing soft contact lenses is a positive experience for the vast majority of children
- While not everything is known about myopia and myopia control, intervention at the earliest opportunity delivers the best effect and all children with myopia should be offered myopia control
This article was supported by an educational grant from CooperVision.
- Professor Debbie Jones is a clinical professor at the University of Waterloo, Waterloo, Ontario, Canada and clinical scientist at the Centre for Ocular Research & Education.
- Professor Nicola Logan is a professor of Optometry and Physiological Optics at the School of Optometry, Aston University, Birmingham, UK.
References
- Holden, BA, et al, Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology, 2016. 123(5): p. 1036-42.
- Jonas, JB, et al, IMI Prevention of myopia and its progression. Investigative Ophthalmology & Vision Science, 2021. 62(5): p. 6.
- Chamberlain, P, et al, Long-term effect of dual-focus contact lenses on myopia progression in children: A 6-year multicenter clinical trial. Optometry & Vision Science, 2022. 99(3): p. 204-212.
- Chamberlain, P, et al, A 3-year randomized clinical trial of MiSight lenses for myopia control. Optometry & Vision Science, 2019. 96(8): p. 556-567.
- Chamberlain, P and B Arumugam, Myopia progression on cessation of Dual-Focus contact lens wear: MiSight 1 day 7-year findings. Optometry & Vision Science, 2021. 98(210049).
- Chamberlain, P, et al, Axial length targets for myopia control. Ophthalmic & Physiological Optics, 2021. 41(3): p. 523-531.
- Arumugam, B, et al, Modelling age effects of myopia progression for the MiSight 1 day clinical trial. Investigative Ophthalmology & Vision Science, 2021. 62(8 2333).
- Flitcroft, DI, The complex interactions of retinal, optical and environmental factors in myopia aetiology. Progress in Retinal and Eye Research, 2012. 31(6): p. 622-60.
- Jones-Jordan, LA, et al, Myopia progression as a function of sex, age, and ethnicity. Investigative Ophthalmology & Vision Science, 2021. 62(10): p. 36.
- Chua, SY, et al, Age of onset of myopia predicts risk of high myopia in later childhood in myopic Singapore children. Ophthalmic & Physiological Optics, 2016. 36(4): p. 388-94.
- Gwiazda, J, et al, A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Investigative Ophthalmology & Vision Science, 2003. 44(4): p. 1492-500.
- Cheng, D, et al, Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmology, 2014. 132(3): p. 258-64.
- Arumugam, B, P Chamberlain, and A Bradley, The effects of age on myopia progression with dual-focus and single vision daily disposable contact lenses. Optometry & Vision Science, 2020. 97(e-abstract 205340).
- Brennan, NA, et al, Efficacy in myopia control. Progress in Retinal and Eye Research, 2021. 83: p. 100923.
- Group, C, Myopia stabilization and associated factors among participants in the Correction of Myopia Evaluation Trial (COMET). Investigative Ophthalmology & Vision Science, 2013. 54(13): p. 7871-84.
- Ruiz-Pomeda, A, et al, Rebound effect in the Misight Assessment Study Spain (Mass). Current Eye Research, 2021. 46(8): p. 1223-1226.
- Hammond, D and B Arumugam, Myopia control treatment gains are retained after termination of dual-focus contact lens wear with no evidence of a rebound effect. Optometry & Vision Science, 2021. 98.
- Tideman, JW, et al, Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmology, 2016. 134(12): p. 1355-1363.
- Sulley A, Wearer experience and subjective responses with dual focus compared to spherical, single vision soft contact lenses in children. Optometry & Vision Science, 2019. 96.
- Walline, JJ, et al, Benefits of contact lens wear for children and teens. Eye & Contact Lens, 2007. 33(6 Pt 1): p. 317-21.
- Rah, MJ, et al, Vision specific quality of life of pediatric contact lens wearers. Optometry & Vision Science, 2010. 87(8): p. 560-6.
- Woods, J, et al, Ocular health of children wearing daily disposable contact lenses over a 6-year period. Contact Lens & Anterior Eye, 2021. 44(4): p. 101391.
- Chalmers, RL, et al, Adverse event rates in the retrospective cohort study of safety of paediatric soft contact lens wear: the ReCSS study. Ophthalmic & Physiological Optics, 2021. 41(1): p. 84-92.