The BCLA CLEAR medical use of contact lenses publication provides a brief introduction to the types of contact lenses used in a medical setting and also defines certain relevant terminology.1 The report proposes the following definition for a medical contact lens – a ‘contact lens that is worn for the primary purpose of treating an underlying disease state or complicated refractive status.’
The two subcategories of medical contact lenses are:
- Therapeutic contact lenses, also known as bandage contact lenses (BCLs) - defined as ‘lenses that are used for the treatment of ocular discomfort or to support the cornea during healing after surgery or when the cornea is being treated for an underlying disease state or to protect the cornea from the environment or mechanical interaction with the lids’
- Rehabilitative contact lenses - defined as ‘lenses that are prescribed for conditions that prevent a patient from achieving adequate visual function with spectacles because of high, irregular, or asymmetric refractive error. Partially or completely occlusive lenses that improve function or cosmesis after trauma, surgery, or stroke also fall into this category’
The table below summarises the indications for each use of medical contact lens, which will be discussed in more detail in the following sections.
Table 1: Indications for the use of medical contact lenses
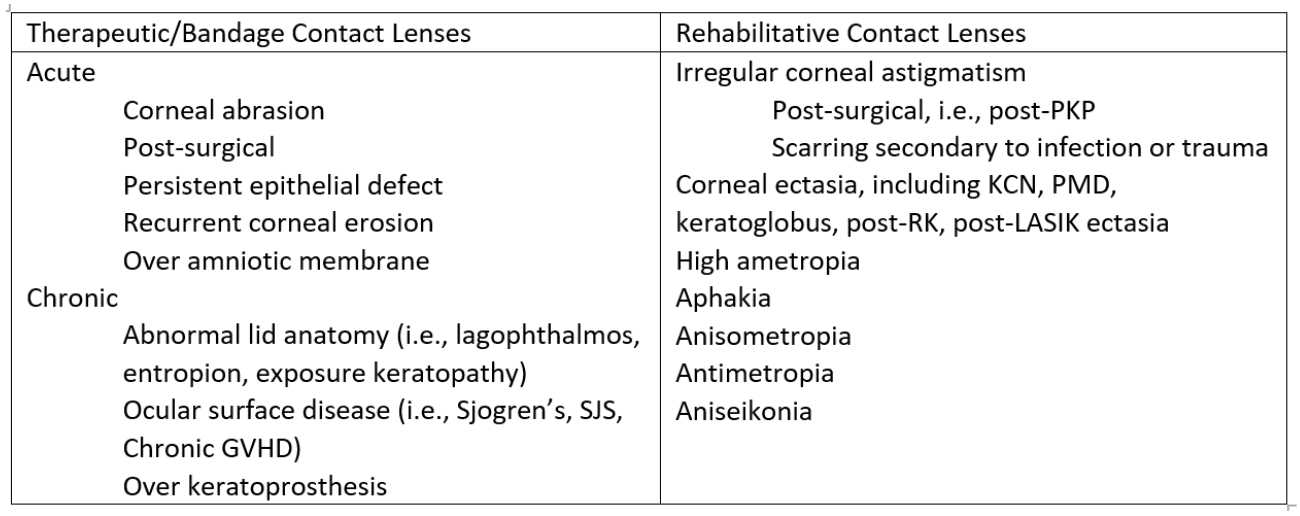
RK = radial keratotomy; LASIK = laser assisted in situ keratomileusis; PKP = penetrating keratoplasty; SJS = Stevens-Johnson Syndrome; GVHD = Graft versus host disease
Bandage lenses in acute setting
As listed in table 1, therapeutic contact lenses play a vital role in the management of acute ocular surface disease and/or corneal epitheliopathy.
Post-surgical
The report discusses in detail the variety of surgeries that use therapeutic contact lenses to improve healing and provide improved comfort to the patient after the procedure. Evidence is cited of the safe and effective use of BCLs after the following procedures:
- Photorefractive keratectomy (PRK)
- Laser epithelial keratomileusis (LASEK)
- Phototherapeutic keratectomy (PTK)
- Epithelial-off corneal crosslinking (CXL)
- Ethylenediamine-tetra-acetic acid (EDTA) treatment for band keratopathy
- Phacoemulsification
- Ptosis repair
- Bleb leaks, perforations and penetrating wounds
On the other hand, a summary of only equivocal evidence is cited for the use of therapeutic contact lenses after penetrating keratoplasty and pterygium repair.
Medical contact lenses
- Contact lens that are worn for the primary purpose of treating an underlying state or complicated refractive status
Bandage contact lenses
- Post cornea, lens extraction or eyelid surgery to improve healing and comfort
- For protection for those with corneal epithelial damage from corneal abrasions, epithelial defects or recurrent corneal erosions
Post-epitheliopathy
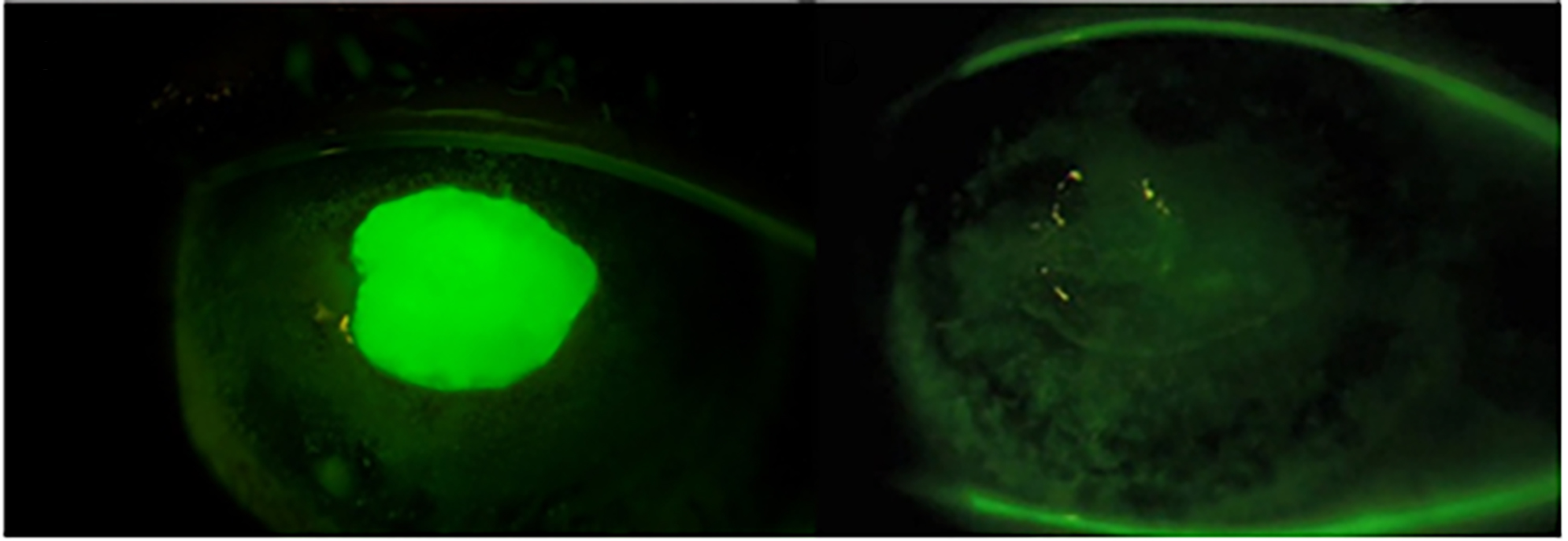
Therapeutic lenses assist in the healing of acute epithelial damage by providing protection from external environmental factors as well as the mechanical interaction of the lids. By doing so, these lenses provide an environment in which the corneal tissue can heal without excessive desiccation and/or shearing forces from blinking, both of which can deter healing. This indication is relevant in certain clinical situations, including after persistent epithelial defects, recurrent corneal erosions, corneal abrasions and over tissue adhesives after corneal perforations or over amniotic membranes.
Figure 1 A: (left) Persistent epithelial defect secondary to neurotrophic keratopathy from Herpes simplex virus. B. (right) Lesion healed after scleral lens wear. (Image courtesy of Karen G Carrasquillo)
Contact Lenses for Chronic Disease
Based on the substantial evidence and literature, there are several chronic conditions discussed that are managed with contact lenses for medical use. These are outlined below in Table 2: Chronic ocular surface disease conditions that may benefit from medical contact lenses:
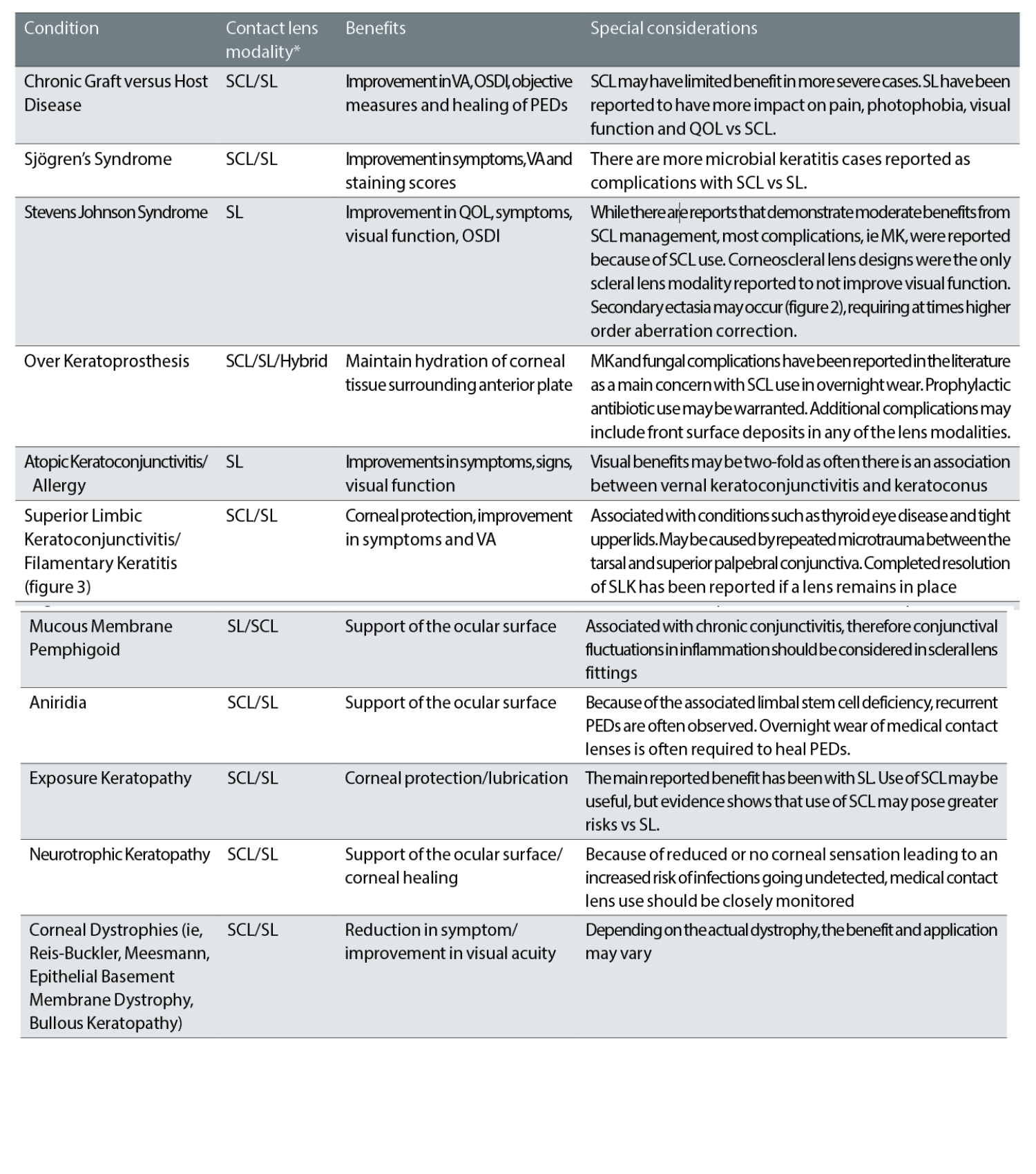
SCL = soft contact lens; SL = scleral lens; VA = visual acuity; OSDI = ocular surface disease index; QOL = quality of life; MK = microbial keratitis;
PEDs = persistent epithelial defects
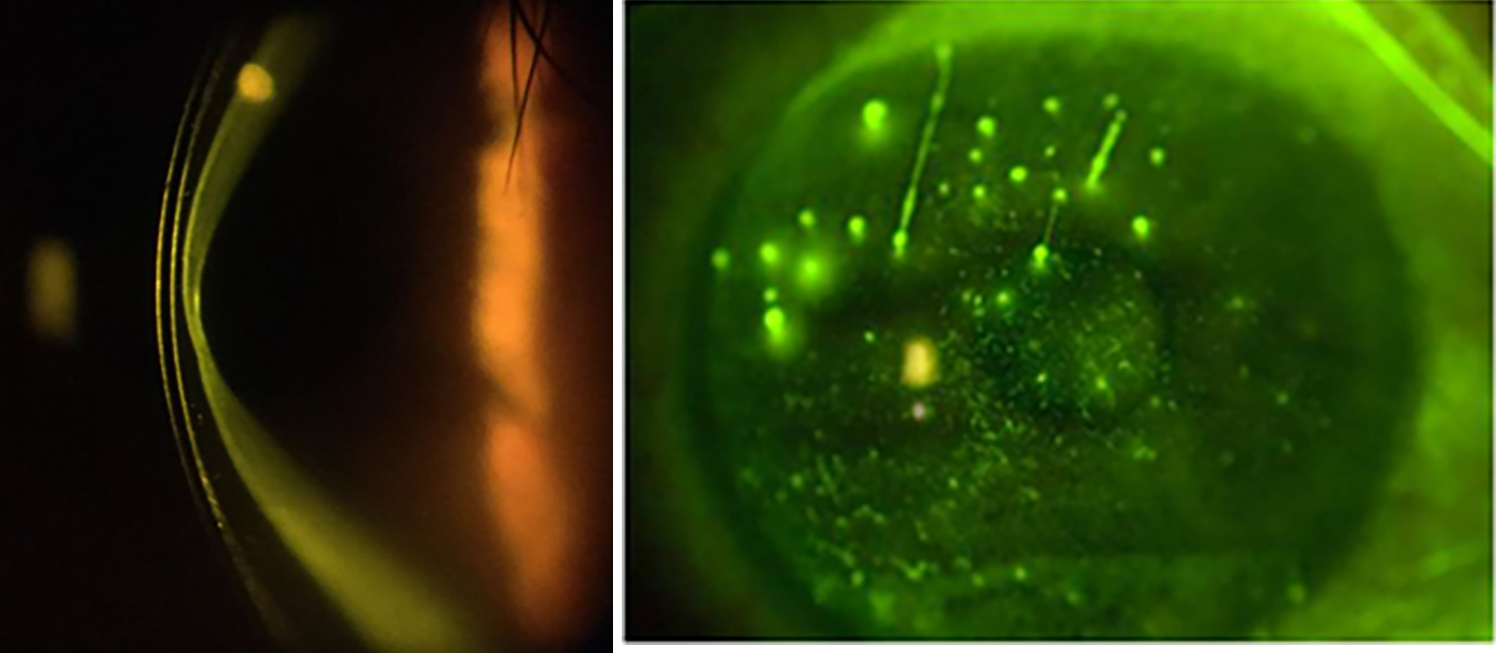
Figure 2 & 3: Secondary ectasia in Stevens-Johnson Syndrome. (Image courtesy of Karen G Carrasquillo); Filamentary keratitis in GVHD. (Image courtesy of BostonSight)
Contact lenses for visual rehabilitation
In some ocular pathologies, conventional corrective methods, such as glasses or conventional contact lenses, fail to provide the patient with functional vision. In these cases, medically necessary contact lenses can be vital for visual rehabilitation to provide the best visual function and quality of life.
A variety of contact lens types may be used depending on the condition, the severity of the disease, and the ability to reach a physiologically compatible and stable fitting lens. The categories of medically necessary contact lenses include:
- Rigid corneal lens (RCL)
- Specialty soft lens
- Hybrid lens (with a RCL centre and a soft skirt)
- Piggyback (a RCL fit over and on top of a soft contact lens)
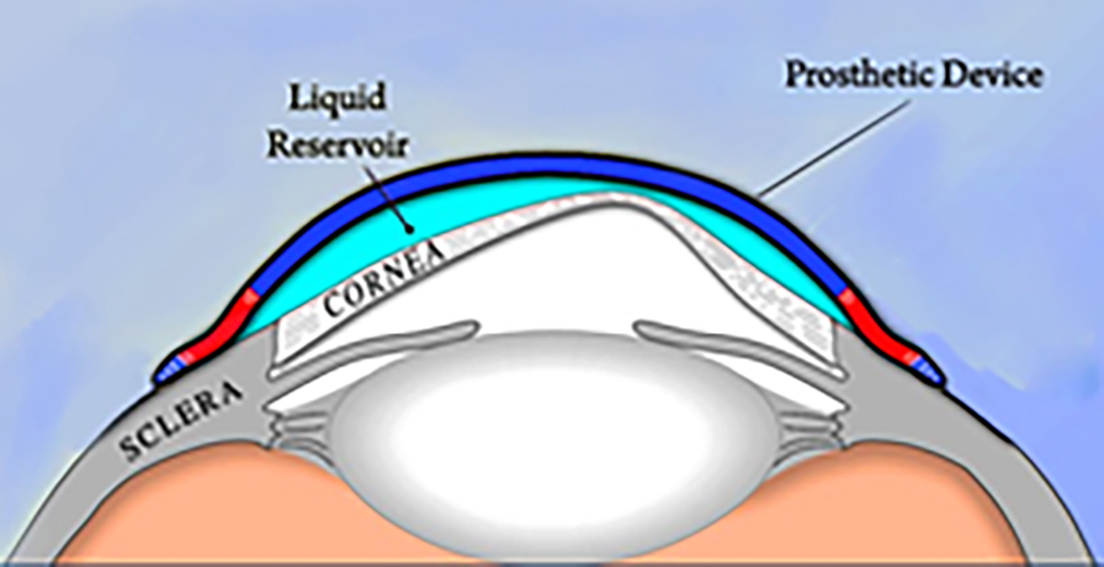
- Scleral lenses (figure 4)
A large subgroup of patients that benefit from contact lenses for visual rehabilitation are those with corneal ectasias and/or irregular corneal astigmatism (see table 3). These patients can suffer from poor visual acuity and function due to the irregular shape of the cornea. Rigid lenses such as RCL or scleral lenses can provide patients with improved vision by masking the underlying irregular cornea and providing a new and regular refractive front surface for the optical system.
Figure 4: Schematic of scleral lens over irregular cornea. (Image courtesy of BostonSight)
Patients with high refractive error benefit from contact lenses due to the large prismatic effect and minification or magnification that can occur in glasses for these patients. Similarly, in anisometropic, antimetropic and aphakic patients, contact lenses help reduce prismatic effects and aniseikonia.
Table 3: Comparison of contact lenses for visual rehabilitation
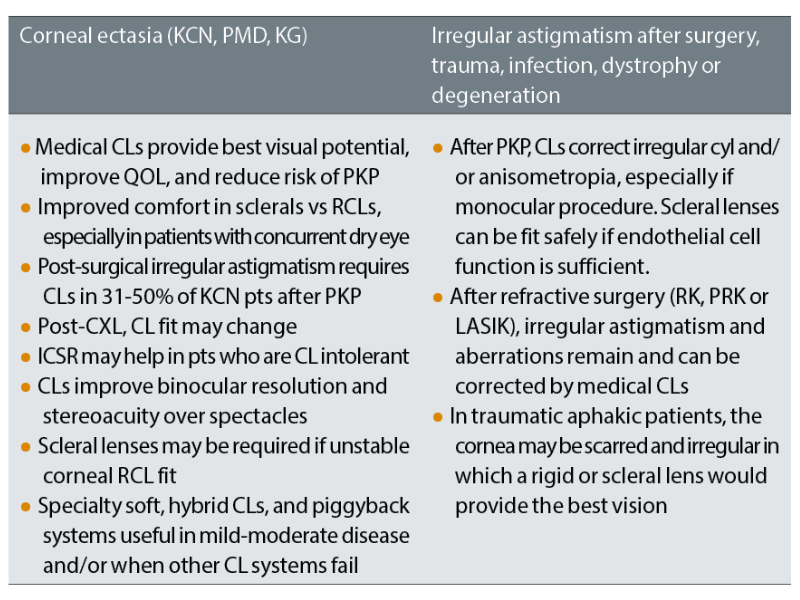
CLs = contact lenses; QOL = quality of life; PKP = penetrating keratoplasty; RCLs = rigid corneal lens; KCN = keratoconus, PMD = pellucid marginal degeneration; KG = keratoglobus; CXL = crosslinking; ICSR = intracorneal stromal rings; RK = radial keratotomy; PRK = photorefractive keratectomy (PRK); LASIK = laser assisted in situ keratomileusis
Tinted opaque or prosthetic lenses
Tinted opaque or prosthetic lenses for medical use can be categorised thus:
- Cosmetic tinted lens; lens that is designed to beautify the appearance of a healthy eye, frequently used to enlarge the pupil or change iris colour.
- Therapeutic tinted lens; treats an ocular disease or defect, can be prescribed for glare, photophobia, to enhance colour vision and for occlusion therapy in amblyopia.
- Prosthetic tinted lens; improve cosmesis for an otherwise cosmetically abnormal eye. Typically used in congenital abnormalities, disfiguring disease, and penetrating trauma.
Medical contact lenses are not only used for refractive error and visual clarity but also for visual comfort. This is particularly important in the case of photophobia and glare after trauma or in the setting of ocular disease such as ocular albinism. Photophobia and glare can affect visual function and quality of life significantly, even if the patient has ‘normal’ visual acuity levels.
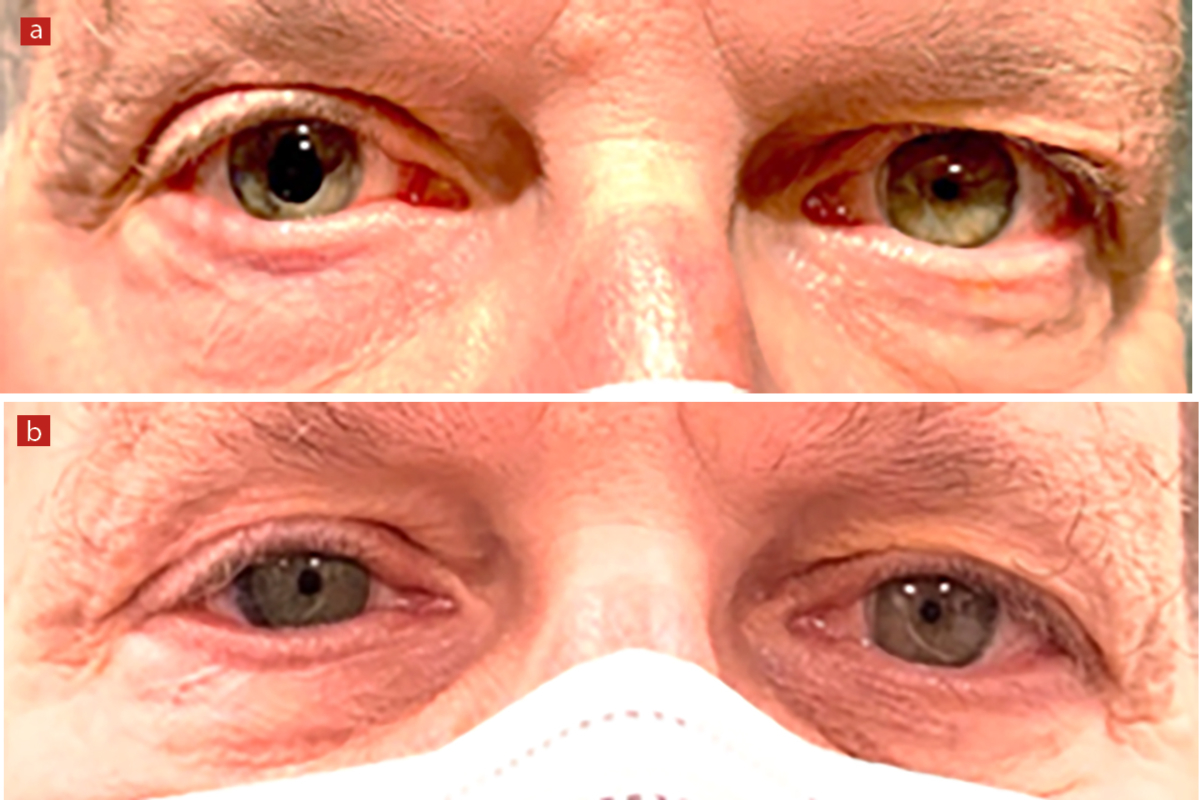
Therapeutic contact lenses have been shown to improve photophobia and quality of life in both adults and children. In some cases, the contact lens is not only reducing photophobia but also improving cosmesis, particularly in cases of disfiguring disease or trauma. Figure 5 is an example of a patient who was successfully fitted in therapeutic tinted soft contact lenses to reduce photophobia after a fixed, surgical peaked pupil in the right eye.
Figure 5 A:. A patient with an irregular pupil following retinal detachment repair surgery in the right eye. Note the peaked, surgical fixed pupil in the right eye on baseline. B. A well colour-matched soft tinted lens was fitted in the right eye with an artificial pupil of the same size to match the left eye for best cosmesis and for best control of the patient’s symptoms of glare. (Images courtesy of Kellen Riccobono)
Examples of conditions in which tinted lenses can be used:
- Retinitis pigmentosa
- Cone dystrophies
- Albinism
- Traumatic aniridia
- Peripheral iridotomy
- Colour blindness
- Disfiguring disease
- Amblyopia occlusive treatment for penalisation of the better seeing eye or in cases of intractable diplopia
Tinted or prosthetic lenses
- Useful for cosmetic reasons to give a more natural eye look for those with abnormalities or to simply beautify the appearance
- Provide relief from symptoms such as glare, photophobia
- As part of management strategies for amblyopia or colour vision enhancement
Oculomotor Dysfunction
Evidence related to the benefits of contact lenses in nystagmus is scarce and equivocal. Most reports are retrospective studies and there is contradicting evidence in the ability of contact lenses to dampen ocular oscillation in nystagmus and improve visual acuity. The one prospective, randomised clinical trial studying the effects of both soft contact lenses and RCL showed there was no benefit in visual acuity or dampening of ocular oscillation.
As it pertains to lid ptosis, at the time of the report’s publication, there is little evidence supporting the role scleral lenses had in managing several types of lid ptosis, including ocular myopathy, complicated ptosis due to long-term RCL wear, phthisis bulbi, and myopathy from Kearns-Sayre syndrome. There have been no long-term reports on the benefits and/or impact of scleral lenses in this setting.
However, in one case report, Phillis et al report on the long-term impact (eight years) of using scleral lenses as a lid crutch to provide lid support in a pediatric case of a paralytic lid ptosis. They increased the sagittal depth and the lens diameter to raise the upper lid and also distribute the weight of the tall lens over a larger surface area and avoid complications of compression and suction.2
Figure 6) A. Paralytic lid ptosis of the left eye. B. Paralytic lid properly supported by a scleral lens used as a lid-crutch. Image courtesy of Karen G Carrasquillo
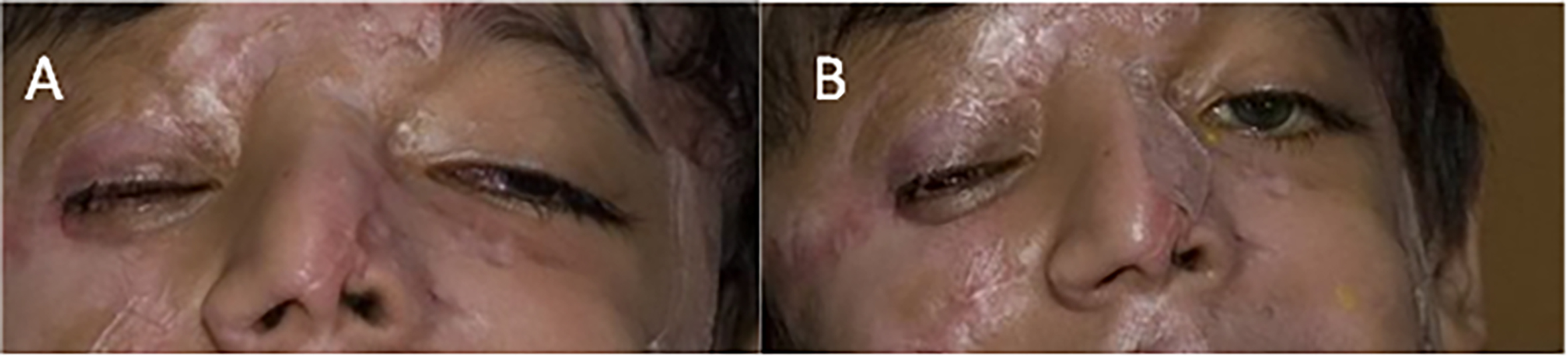
The scleral lens provided adequate visual improvement and lid support, and there were no complications of neovascularisation or edema secondary to the high sagittal depth of the lens. Moreover, they show the cornea has shown signs of clearing in corneal opacities over time, likely from the protection the scleral lens provides against chronic exposure.
Refractive error (high ametropia, antimetropia, anisometropia, aniseikonia, aphakia)
- CLs provide improved vision and better contrast sensitivity over spectacles
- Can use soft or rigid lenses to best correct vision and to avoid amblyopia in pediatric patients
- CLs sometimes used overnight in pediatric patients though risk of MK
- CLs especially important in unilateral conditions, where aniseikonia may be pronounced
- Occlusive contact lenses can be used for unilateral aphakia when diplopia is present
- CLs improve binocular resolution and stereoacuity over spectacles
Medical use of contact lenses with prophylactic antibiotics
Often medical contact lenses are used to treat anterior segment and corneal pathologies, such as corneal abrasions or persistent epithelial defects, where the risk of infection exists due to the nature of an open wound. In this case, it is standard for practitioners to treat with concurrent prophylactic topical antibiotics, typically those of a preservative-free formulation, especially when using these drops in the fluid bowl of a scleral lens. While this practice is common, at the time of this report, there are no well-controlled human studies to determine the true efficacy.
Though reports of soft lenses pre-soaked in gentamicin were able to provide an inhibitory concentration of gentamicin in the tear film for three days and when a combination was used delivery into the anterior chamber. Much is still to be explored, however prophylactic use of antibiotics typically over a soft contact lens on the eye or inside the scleral lens reservoir before application on eye is often used to reduce the risk of microbial keratitis along with close monitoring.
Medical use of contact lenses during therapy with other agents
This section summarises the reports describing the concurrent use of topical therapeutic agents with contact lenses. Two groups of drugs can be considered:
Corticosteroids and NSAIDs
- Some concerns to use concomitantly with contact lenses, because of potential toxicity
- Additional concerns secondary to risk for infection
- Animal studies have shown that soft contact lenses potentiate the delivery of these into the aqueous humour
Glaucoma medications
- Among the first to be prescribed along with contact lens use
- Preservatives in these can cause corneal toxicity
- Concomitant use of these with contact lenses should be pursued with caution and closely monitored
- Animal studies have shown that soft contact lenses may potentiate the delivery of these agents into the aqueous humour
Complications of medical use of contact lenses
In ocular surface disease, the compromised nature of the ocular surface or the severity of the disease may render these corneas more vulnerable or prone to complications during contact lens wear, including infection and more regular review may be advised.
However, the typical complications and risk factors are largely the same as for those who wear contact lenses for refractive purposes. Overnight lens wear especially if corticosteroids are being taken for example for concomitant inflammatory disease, increases the risk of infection further and the use of antibiotic prophylaxis may be prescribed.
Complications may, in some instances, be precipitated by the underlying disease. For example, corneal melt and perforation has been reported in patients with cGVHD wearing bandage soft contact lenses, however, this complication is likely due to the immune-mediated disease rather than to therapeutic lens wear.
Patient instructions and education in wear and care
The wearer should be educated on all aspects of lens care and handling, regarding application and removal aspects family members may also be trained to provide support (figures 7 and 8). Wearing needs may vary depending on the reason for contact lens use and personal motivation.
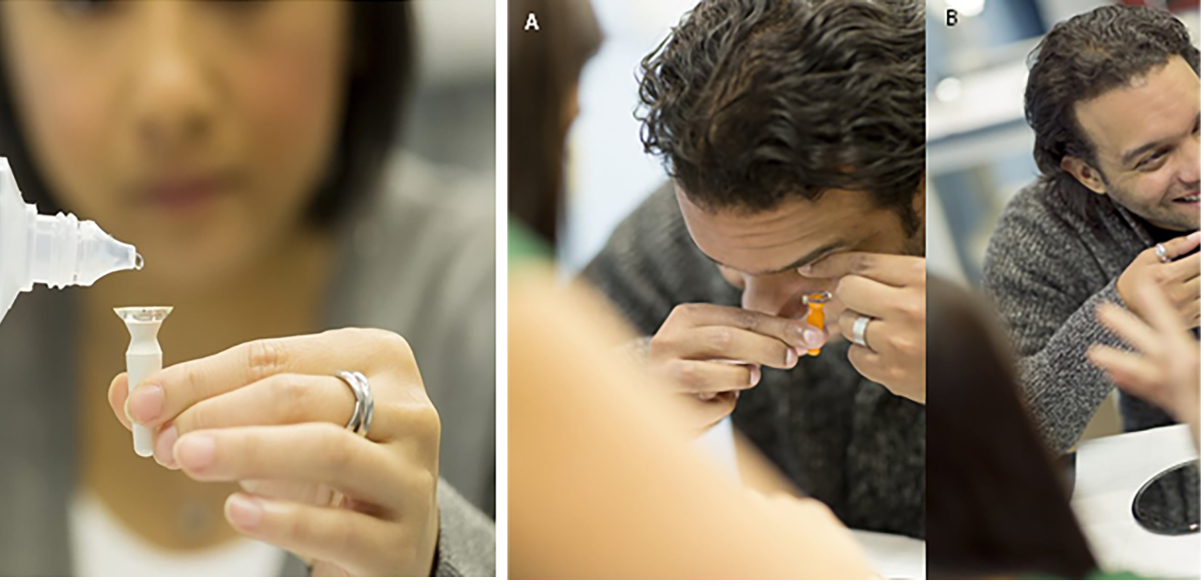
Figure 7 & 8: (Left) Patient filling scleral lens reservoir with preservative-free saline. Preserved solutions are to be avoided for this application. (Right) A. Patient applying scleral lens. B. Patient experiencing relief in pain and photophobia after lenses were applied; an example of how these lenses have a positive impact in patient’s quality of life. (Pictures courtesy of BostonSight)
As far as disinfection regimen, even though traditional gas permeable lens products consist of preserved multipurpose solutions, when using medical contact lenses to manage ocular surface diseases, the preservatives in these solutions may cause hypersensitivity reactions. Therefore, preservative-free solutions may be preferred, ie a hydrogen peroxide-based cleanser.
Compliance is another important aspect in the use of medical contact lens in order to minimise and/or avoid complications. Education is important and regular review to maximise success and reduce risk.
When it comes to the patient experience when using contact lenses for medical use, the evidence is overwhelmingly positive when it comes to scleral lenses, with numerous studies reporting on the improvement in quality of life, activities of daily living, and visual function, among others. The same applies to soft contact lenses when used as bandage lenses, although not as overwhelmingly as scleral lenses.
Wearing schedules
- Most patients requiring medical contact lenses often wear them every waking hour
- Various retrospective studies report the average scleral lens wear time to be ~12h
- Overnight wear of therapeutic soft contact lenses (silicone hydrogels) or scleral lenses may be warranted at times. In each scenario, careful monitoring is required
Five clinical pearls
- Medical contact lenses for visual rehabilitation in the case of corneal disease can provide a significant improvement in visual acuity, visual function, and quality of life
- Contact lenses can be used as a bandage to the ocular surface to treat epithelial erosions, abrasions, or persistent defects to improve healing and patient comfort
- Tinted contact lenses can be beneficial not only in the management of photophobia or glare but also in the improvement of cosmetic appearance after trauma and/or surgery
- Proper management and monitoring for adverse events such as microbial keratitis with medical contact lenses is vital
- Soft lenses may potentiate the delivery of topical therapeutics to the ocular surface and the aqueous humour
Conclusion
There are many ways that contact lenses can be used in a medical setting to treat the ocular surface or provide the best possible visual potential. This article will conclude with five clinical pearls related to the material covered above.
- The full report and supplementary information can be accessed at https://doi.org/10.1016/j.clae.2021.02.002
- The BCLA CLEAR Summary report is a short bite-size evidenced based practical guide for clinicians, bringing together the key findings from the report. Accessed via CLEAR (bcla.org.uk)
- Listen to BCLA CLEAR medical use of contact lenses podcast: https://podcasts.apple.com/cz/podcast/bcla-clear-episode-6-medical-use-of-contact-lenses/id1524673927?i= 1000549957771
The editors for this series are Neil Retallic and Dr Debarun Dutta.
Acknowledgements
Acknowledgement and recognition to Deborah S Jacobs, Paul D Cottrell, Fernando J Fernández-Velázques, Raquel Gil-Cazorla, Isabelle Jalbert, Andrew D Pucker, Danielle M. Robertson, Loretta Szczotka-Flynn, Lynne Speedwell, and Fiona Stapleton who were the paper’s authors and to the educational grants from Alcon and CooperVision.
Original paper: Jacobs DS, Carrasquillo KG, Cottrell PD, Fernández-Velázquez FJ, Gil-Cazorla R, Jalbert I, Pucker AD, Riccobono K, Robertson DM, Szczotka-Flynn L, Speedwell L, Stapleton F. BCLA CLEAR – Medical use of contact lenses. Contact Lens & Anterior Eye, 2021 Apr;44(2):289-329.
References
- Jacobs DS, Carrasquillo KG, Cottrell PD, Fernández-Velázquez FJ, Gil-Cazorla R, Jalbert I, et al. BCLA CLEAR – Medical use of contact lenses. Contact Lens & Anterior Eye, 2021;44:289–329. https://doi.org/10.1016/J.CLAE.2021.02.002.
- Phillis K, Brocks D, Carrasquillo KG. Case Report: Use of prosthetic replacement of the ocular surface ecosystem treatment of traumatic lid ptosis in a pediatric patient. Optometry & Vision Science, 2020;97:1029–33. https://doi.org/10.1097/OPX.0000000000001612.