While, at first, this might hardly be considered a topic of everyday concern, a range of issues relating to vision and ocular health have been identified for individuals engaging in space travel. As progressively longer flights into conditions of zero gravity are anticipated, this will increasingly become a focus for associated research and the possible development of systems to minimise the effect of such changes. This area of research is also likely to provide greater understanding of the dynamics of the distribution of cerebrospinal fluid as a feature of typical terrestrial human physiology.
Mir and ISS
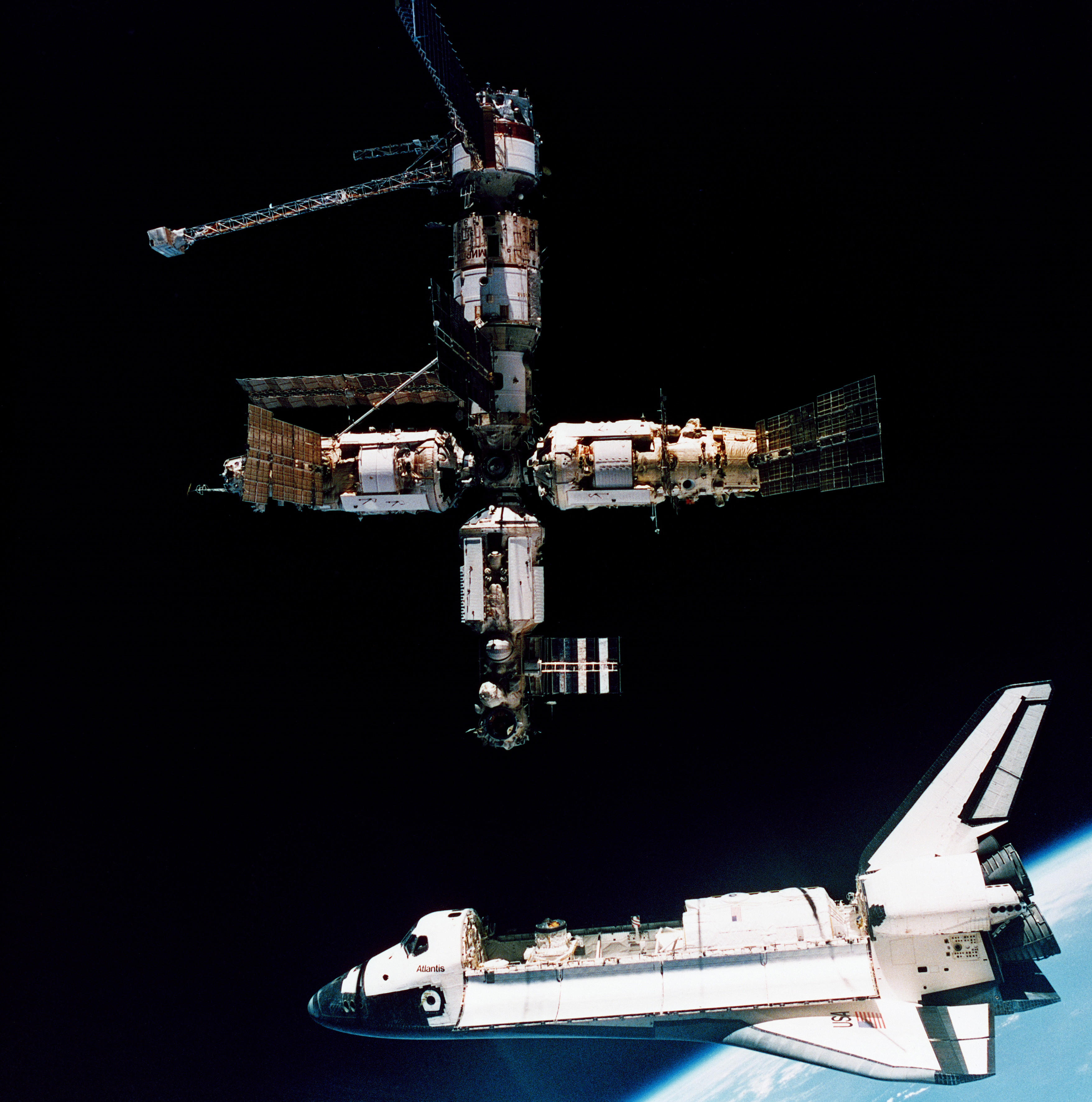
The Mir space station (named from the Russian word for ‘peace’ or ‘world’) was the first permanent earth orbiting platform and became operational in March 1986 with a crew of three. Helen Sharman of the United Kingdom was a crew member of the October 1991 Mir mission and so became the first British person, first Western European woman and first privately funded woman in space. The station was de-orbited in March 2001 when funding was withdrawn. Figure 1 reflects a period of significant co-operation between the USA and Russia in space exploration, with the Space Shuttle allowing supply and replacement of provisions, equipment and crew.
Figure 1: Space shuttle Atlantis undocking from Mir in July 1995. Credit Nasa
The various technologies of Mir were, essentially, fully adopted by and further developed in the International Space Station (ISS). This was ready to receive its first crew members in November 2000 and was configured for a permanent crew of six. Key initial modules of the ISS had, in fact, been designed and constructed for the planned Russian successor station Mir-2 which, due to political and economic developments on Earth, was never built. Without such available existing technology, the ISS would have taken the wider international community significantly longer to construct.
The ISS depended significantly on the Space Shuttle for module assembly and re-supply. This phase came to an end with the retirement of the remaining three Space Shuttles in July 2011. Figure 2 shows the ISS near to completion.
Figure 2: The International Space Station photographed by Expedition 56 crew members from a Soyuz spacecraft after undocking, in October 2018. Credit Nasa

The space stations made it possible to study the impact of low gravity and out-of-atmosphere conditions upon human physiological processes, including those involved with vision.
Initial Observations in Microgravity
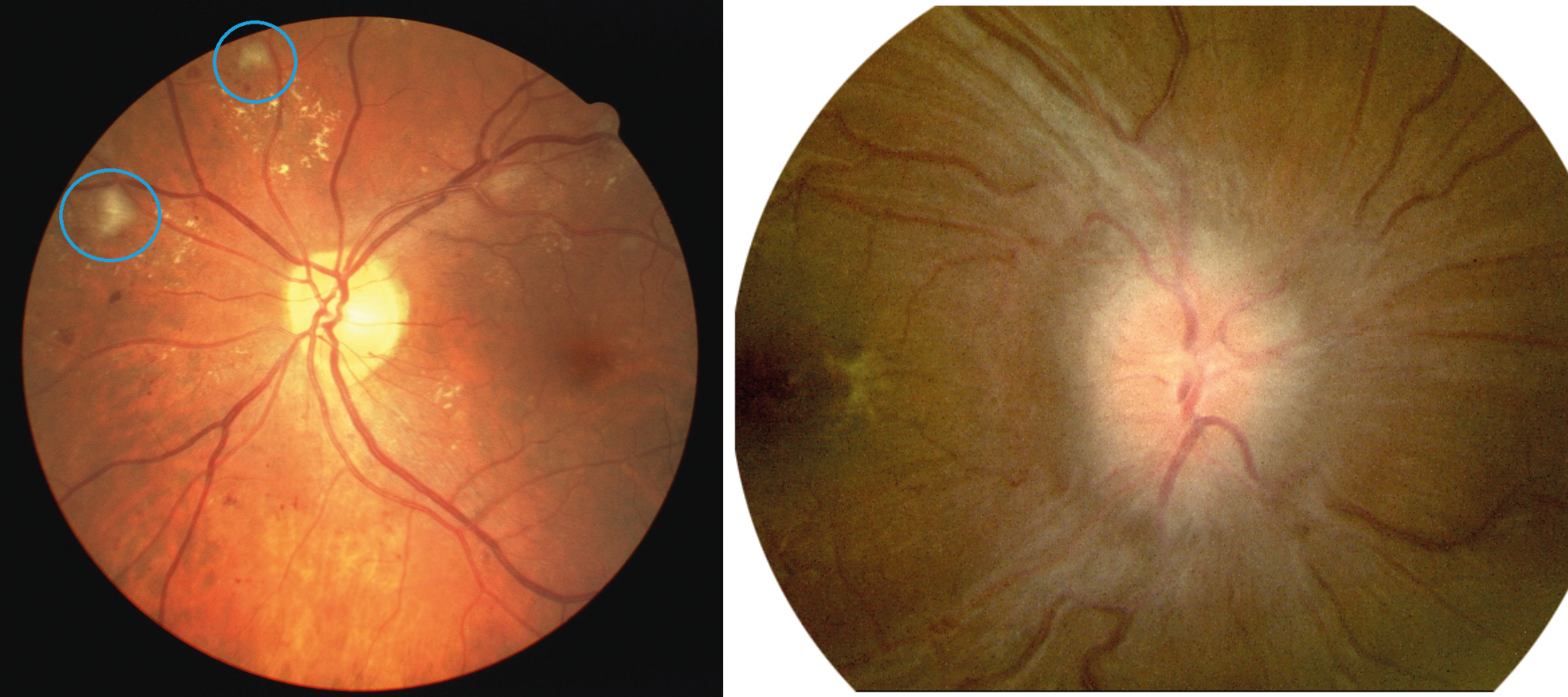
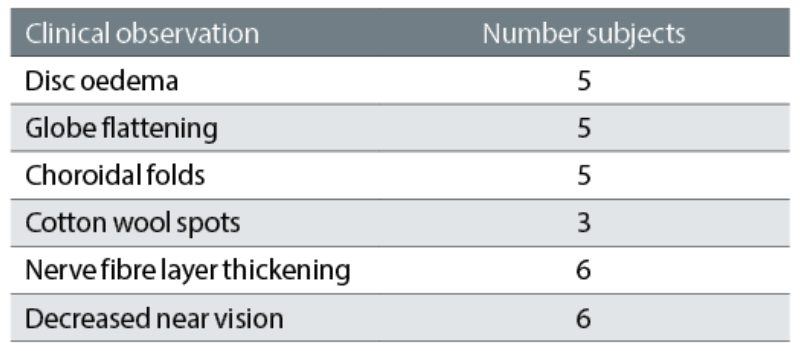
Observations of ocular changes during periods of weightlessness in space were first described by Mader et al in a study that primarily observed changes in the ocular pathology of seven astronauts after an extended period of space flight.1 Table 1 summaries their initial findings, which included cotton wool spots (figure 3), indicative of slowed axoplasmic flow in retinal nerve fibre axons as a result of ischaemia, and disc oedema (figure 4).2,3
Figure 3 & 4: (left) Cotton wool spots indicating areas of ischaemia in a diabetic; (right) Disc oedema
Such initial observations paved the way for more detailed and extensive investigation as it was identified that ocular changes initiated by prolonged weightlessness conditions could present a significant obstacle for future space missions of longer duration. In a review of such early studies, Lee et al described how such ocular changes were initially described as visual impairment and intracranial pressure (VIIP) syndrome, and it was conjectured that such ocular changes were likely to be triggered by elevated intracranial pressure.4
Table 1: Initial observations described by Madder et al1 of changes in ophthalmic parameters after significant exposure to micro-gravity
It was also commented that observations of the ocular status of astronauts due to periods of weightlessness on the ISS were made more difficult by the typical delay in recovering the crew from Russian Soyuz re-entry modules after often traumatic landings in Kazakhstan.
Idiopathic Intracranial Hypertension
The term idiopathic intracranial hypertension (IIH) is used to describe elevated intracranial pressure related to cerebrospinal fluid volume changes and has been identified as a condition mostly affecting young, often obese, women of child-bearing age. It may present with a range of symptoms, including headache, and there is an association between the degree of swelling of the optic nerve and the extent of any visual loss.5, 6
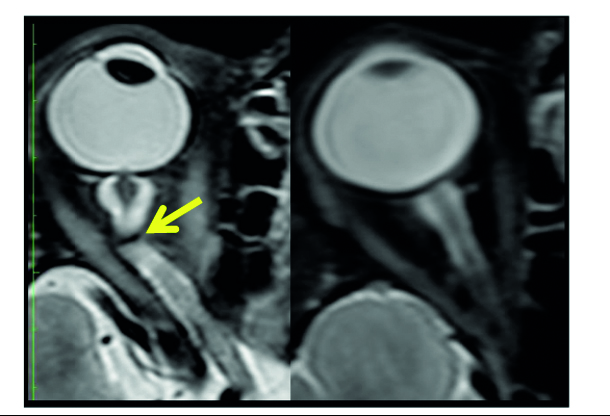
Various treatment strategies have been developed over time, though the Idiopathic Intracranial Hypertension Treatment Trial7 confirmed the benefits of a weight-reduction programme combined with a low-sodium diet in association with the use of the carbonic anhydrase inhibiting drug acetazolamide. Ocular changes associated with IIH, in addition to the optic nerve head swelling, include optic nerve tortuosity and optic nerve sheath distension. Optic nerve tortuosity may be identified by a buckling of the retrobulbar optic nerve pathway and may be readily observed in MRI images (figure 5).
Figure 5: Kinking of the retrobulbar optic nerve pathway. Credit Nasa
The environment of space makes direct measurement of intracranial pressure impractical in order to confirm the cause of suspected VIIP syndrome. Using a novel approach, however, Lawley et al used the zero gravity achievable during parabolic flight to make a series of observations of intracranial pressure in a number of volunteers.8 These volunteers had catheters, of a design previously used for the delivery of prophylactic chemotherapy, inserted into their lateral ventricle. A series of measurements of intracranial pressure were made at zero gravity and also in terrestrial based subjects, both sitting in upright and supine positions.
It was confirmed that, in the terrestrial seated position, the intracranial pressure measured in all subjects was around 4mmHg while, in the supine position, was around 15mmHg. In microgravity in the supine position, the pressure was recorded to be around 13mmHg, so slightly less than equivalent terrestrial supine values. The inference drawn from this is that microgravity does not elevate intracranial pressure values unduly. Such observations also indicated that, in normal daily terrestrial activity, the intracranial pressure levels vary between a lower value consistent with sitting upright and a higher value when in the supine position, though no pathologies are considered to arise from this exposure.
Spaceflight Associated Neuro-Ocular Syndrome
The realisation that excessive intracranial pressures were not experienced during microgravity subsequently led to the defining of a subset of ophthalmic abnormalities linked to spaceflight, which came to be described as spaceflight associated neuro-ocular syndrome, or SANS.9 The various components of SANS are summarised in table 2.
Table 2: Main features of spaceflight associated neuro-ocular syndrome (SANS)
Ophthalmic Observations on the ISS
A better understanding of the vision changes that result from prolonged exposure to microgravity on the ISS has been facilitated by comparing the results from tests carried out before missions, during missions and after missions. This has made it possible to identify the relative permanence of any of the observed changes and has also led to the development of various modes of vision testing aboard the ISS. The vision monitoring programme on board the ISS summarised in table 3 and shows how ISS astronauts are probably the most intensely monitored group of scientific personnel on (or off) the planet with regard to ophthalmic parameters.
Table 3: Summary of eye and vision test systems on the ISS
One key development within this programme was the deployment of OCT within the ISS, initially a Heidelberg Spectralis 1 device in December 2013. This was subsequently upgraded to an OCT2 system in May of 2018. ‘By implementing the next-generation Spectralis OCT2 Module, Nasa will be able to take an even deeper dive into understanding space flight associated neuro-ocular syndrome (SANS),’ said Dr David M Brown, the retina specialist on the Nasa SANS Research and Clinical Advisory Panel at the time of the OCT2 upgrade.
‘In response to the conditions of long duration space flight, the eyes of almost all of our astronauts experience swelling in the blood supply layers (the choroid) behind the retina and swelling of the optic nerve as it enters the eye. The Spectralis OCT2 Module will enable imaging of these deeper layers of the choroid and optic nerve throughout the space flight and upon the astronauts’ return to Earth’s gravity. Discovering the underlying mechanism of SANS will be mission critical to develop countermeasures necessary for planned spaceflights to Mars and beyond.’
All such measurements undertaken on the ISS are typically co-ordinated with ground-based specialist technicians in order to ensure consistent quality of data.
Figure 6: Avia Tonopen

Fruits of Research
Investigations into the nature of SANS have utilised ‘before’ and ‘after’ spaceflight mission MRI scans to check for changes to optic nerve tortuosity and optic nerve sheath distension. In a study of 10 astronauts who completed ISS missions of typical six months duration, undertaken by Rohr et al, no significant changes to key parameters were observed.10 This suggested that intracranial pressure was not pathologically elevated during spaceflight.
Pre and post-ISS mission observations of total retinal thickness of the 19 ISS crew members, using OCT, and their lateral ventricle volume, using MRI, have been reported by Marshall-Goebel et al.11 An average 4.7μm increase in postflight total retinal thickness was observed with an average 1-mL postflight increase in lateral ventricle volume. The authors commented that microgravity-induced fluid redistribution in space may be a common stressor to the brain and retina.
Sater et al reported the results of a study of globe flattening in the eyes of 10 ISS astronauts for a range of mission durations using a 3 Tesla Siemens MRI scanner.12 Pre-flight data were compared with post-flight observations up to 368 days after end of mission, the first post-mission observation being made around four days after return to Earth. Specialist software was utilised to create a three-dimensional representation of vitreous volumes. A degree of globe flattening was observed in all subjects, though the corresponding vitreous volume change was not significant (at around 0.2%). Such changes reduced after mission completion, but were still detectable up to a year later.
Using the OCT facilities on board the ISS, in addition to ground-based systems, Ferguson et al reported a data set relating to 36 astronauts, which was reviewed for any indication of the development of chorioretinal folds under microgravity conditions.13 Scans were examined for the qualitative presence of chorioretinal folds by a panel of experts. Chorioretinal folds were observed in six crew members and these were identified as a potential useful marker for the evaluation of future counter measures for SANS.
It has long been known that subjects exposed to bed rest will subsequently show an increase in intracranial pressure the following day. A study was undertaken by Laurie et al, using a modified bed rest protocol approved by Nasa where subjects were exposed to a strict negative 6° head-down tilt bed rest for 30 days.14 Observations of optic disc oedema and choroidal engorgement were compared with a group of 20 ISS astronauts over a comparable time period. It was observed that peripapillary total retinal thickness increased to a greater degree among the 11 terrestrial subjects compared with the ISS crew, where an average group difference of 37 microns was identified.
No change in choroidal thickness was observed for subjects exposed to bed rest, though an increase was observed for the ISS crew astronauts as evident in an average 27 micron mean difference between the two groups. The bed rest model, however, is described as having relevance to simulate conditions of microgravity and where the higher peripapillary retinal thickness increase is attributed to the greater elevation of intracranial pressure with strict bed rest.
While MRI imaging is typically used to image physical structure of neural tissue, the use of quantitative magnetic resonance imaging (qMRI) with diffusion tensor imaging (DTI) functionality15 allows the visualisation of neural connectivity within brain structures. This is analogous to viewing the wiring connections in an electronic circuit. The use of this tool is described by Hasan et al as a means of identifying the structural features of the brain compartments of 10 ISS crew members.16 A surprising observation was that the connection patterns observed and the spatial development of specific regions suggested that astronauts develop and maintain cerebral activity consistent with younger, fitter brains.
Greenwald et al identified that microgravity caused a slight increase in intraocular pressure compared to terrestrial values and could be slightly reduced by wearing lower body negative pressure (LBNP) cuffs set at a pressure of 25mmHg.17 Thus, changes in intraocular pressure are not considered significant for the development of SANS symptoms. What might be relevant would be to repeat the experiments of Lawley et al to investigate the effects of LBNP cuffs on intracranial pressure using zero gravity parabolic flight.8
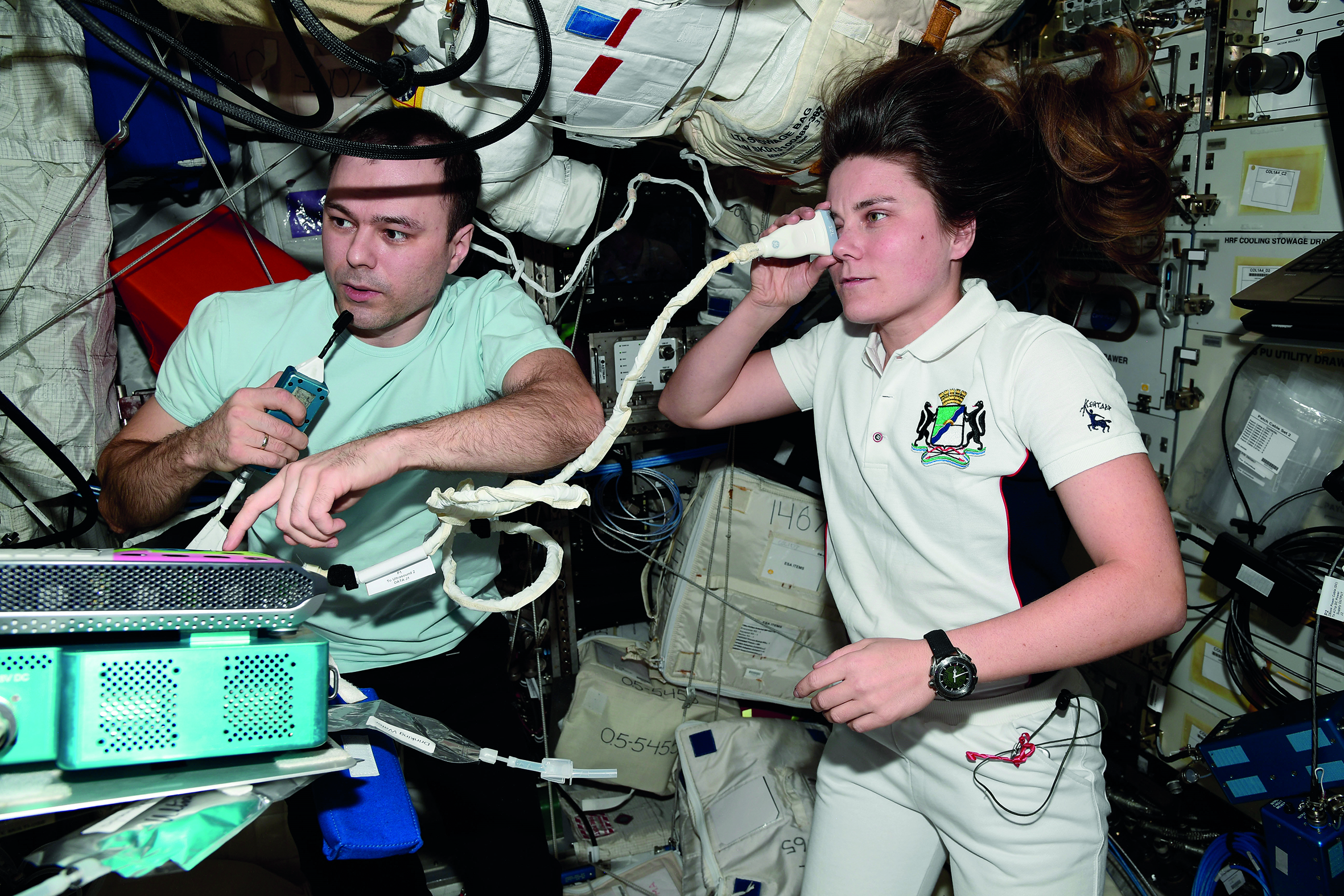
Figure 7: 2023 Expedition 68 flight engineers Dmitri Petelin and Anna Kikina, both from Roscosmos, participate in ultrasound eye scans aboard the International Space Station using the Ultrasound 2 device located in the Columbus laboratory module. Credit: Roscosmos
Pathogen Risks
Documented accounts of the experiences of astronauts on the MIR and ISS space stations indicate the many factors to which they were exposed. This adds complication to the understanding of associated health impacts of microgravity. The diurnal cycle, for example, is absent and replaced by multiple periods of light and dark of multiple orbits during each earth ‘day’. The growth of fungi and other microorganisms in such enclosed environments exposes occupants to additional potential hazards. These include endotoxins in the managed atmosphere.
Various commentators have referenced the potential microbiological hazard of development of ‘exotic’ organisms in the microgravity environment that may pose a threat to the on-board astronauts, and subsequently to the wider human community. Singh et al report DNA analysis of specific strains of Enterobacter bugandensis bacteria, identified on board the ISS.
Several strains with multiple antibiotic resistance were identified with known occurrence in ‘terrestrial’ patients, though other strains were also identified with unknown resistance patterns.18 It was also identified that on-board DNA analysis of strains would improve the confidence level of such observations, due to the extreme environments experienced by organism samples on return to Earth.
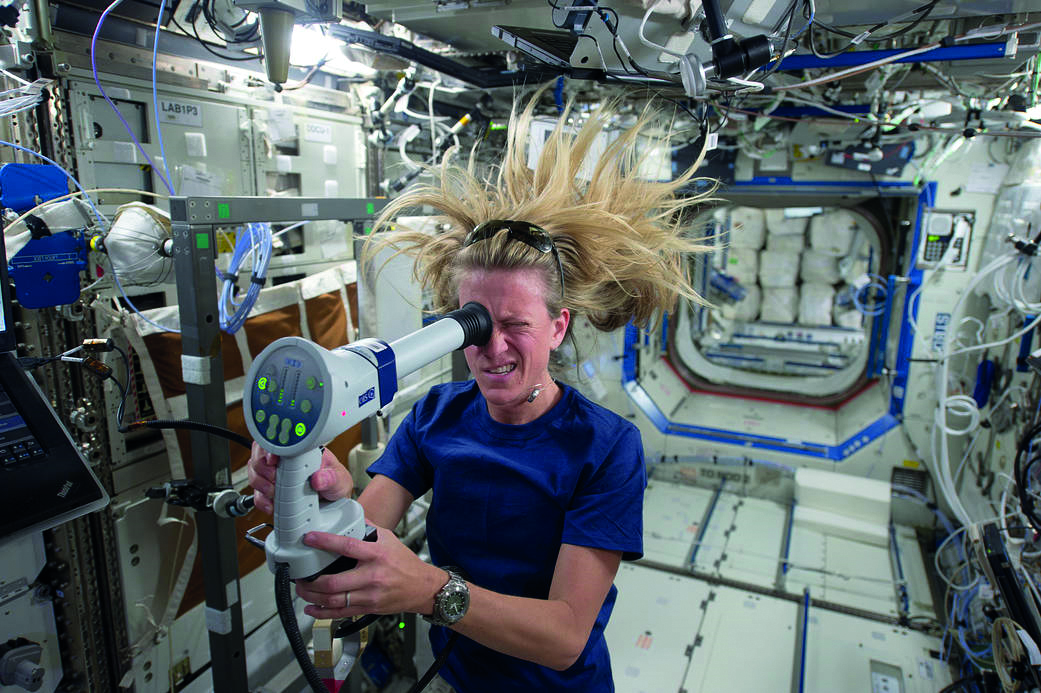
Figure 8: Nasa astronaut and flight engineer Karen Nyberg, of Expedition 36 in 2013, conducts an ocular health exam on herself using a fundoscope in the Destiny laboratory of the Earth-orbiting International Space Station. Credit: Nasa
Physical Eye Models
One novel approach to investigation of the effect of microgravity on the human visual system has been to create a terrestrial-based model of anterior and posterior eye segments and to introduce variations in intraocular pressure and intracranial pressure to observe changes in posterior anatomy. Such a system is described as a translaminar autonomous system (TAS).19
The posterior section of such a model is derived from an enucleated eye, where cell pathology is maintained for periods of up to 14 days by means of neurobasal perfusion medium.20 Pressure within each compartment may be established and maintained by regulated fluid flow and a range of set pressures selected to represent a range of scenarios. No details, however, are provided of temperature range to which the various models were exposed. Detailed analysis was undertaken of various tissues after the 14-day study period. Further work is proposed using the TAS system, including a routine that replicates the pressure dynamics of terrestrial based subjects exposed to supine and proline positions.
One initial explanation of SANS is that, on Earth, the reduction of cerebrospinal fluid associated with the sitting terrestrial position offsets the increase in intracranial pressure associated with the reclining terrestrial position and that, in microgravity conditions, such a compensating factor is absent.
Figure 9: European Space Agency astronaut and flight engineer Alexander Gerst, of Expedition 40 in 2014, uses the Spectralis OCT during an ocular health vision test in the Harmony node of the International Space Station. Credit: Nasa

Cataract
Initial studies of the impact of increased exposure to cosmic radiation among astronauts suggested an increased risk of the primary types of cataracts, and nuclear cataract alone, for astronauts with higher lens exposure. However, later studies of US astronauts reported a higher risk of cortical cataract and posterior subcapsular cataract, but not for nuclear cataract, leading some to suggest the cataract was more likely due to differences in oxygen levels in the space vehicle environments. Further studies, therefore, are required for a better understanding of the progression of cataractogenesis on long-duration missions to the Moon and Mars.21
Summary
The set of observations associated with SANS is a key element of assessment of vision changes induced by micro-gravity on board the ISS. While data is available for periods of weightlessness of up to a year, exposure to periods longer than this is an unknown quantity. While various theories have been identified as to the cause of SANS, the range of investigations undertaken has expanded the understanding of the neuro-ocular environment with potential benefit for terrestrial based eye conditions. The range of investigations, however, has fully exercised scientific innovation and where in particular the study undertaken by Lawley et al made significant findings regarding the likely levels of intracranial pressure in microgravity.8
- Dr Douglas Clarkson is a research fellow at the Department of Clinical Physics and Bioengineering, Coventry and Warwickshire University Hospital Trust.
References
- Mader TH, Gibson CR, Pass AF, Kramer LA, Lee AG, Fogarty J et al. Optic disc edema, globe flattening, choroidal folds, and hyperopic shifts observed in astronauts after long-duration space flight. Ophthalmology. 2011 Oct;118(10):2058-69
- Zhang L, Xu L, Zhang JS, Zhang YQ, Yang H, Jonas JB et al. Cotton-wool spot and optical coherence tomography of a retinal nerve fiber layer defect. Archives of Ophthalmol. 2012 Jul;130(7):913
- Ioannides A, Georgakarakos ND, Elaroud I, Andreou P. Isolated cotton-wool spots of unknown etiology: management and sequential spectral domain optical coherence tomography documentation. Clinical Ophthalmol0gy, 2011;5:1431-3
- Lee AG, Mader TH, Gibson CR, Brunstetter TJ, Tarver WJ. Space flight-associated neuro-ocular syndrome (SANS). Eye (Lond). 2018 Jul;32(7):1164-1167
- Raoof N, Hoffmann J. Diagnosis and treatment of idiopathic intracranial hypertension. Cephalalgia. 2021 Apr;41(4):472-478
- Wall M. Update on Idiopathic Intracranial Hypertension. Neurology Clinic. 2017 Feb;35(1):45-57
- Wall M, McDermott MP, Kieburtz KD, Corbett JJ, Feldon SE, Friedman DI et al. Effect of acetazolamide on visual function in patients with idiopathic intracranial hypertension and mild visual loss: the idiopathic intracranial hypertension treatment trial. JAMA. 2014 Apr 23-30;311(16):1641-51
- Lawley JS, Petersen LG, Howden EJ, Sarma S, Cornwell WK, Zhang R et al. Effect of gravity and microgravity on intracranial pressure. J Physiol. 2017 Mar 15;595(6):2115-2127
- Ong J, Mader TH, Gibson CR, Mason SS, Lee AG. Spaceflight associated neuro-ocular syndrome (SANS): an update on potential microgravity-based pathophysiology and mitigation development. Eye (Lond). 2023 Apr 18.
- Rohr JJ, Sater S, Sass AM, Marshall-Goebel K, Ploutz-Snyder RJ, Ethier CR et al. Quantitative magnetic resonance image assessment of the optic nerve and surrounding sheath after spaceflight. NPJ Microgravity. 2020 Oct 8;6:30
- Marshall-Goebel K, Macias BR, Kramer LA, Hasan KM, Ferguson C, Patel N et al. Association of Structural Changes in the Brain and Retina After Long-Duration Spaceflight. JAMA Ophthalmology, 2021 Jul 1;139(7):781-784
- Sater SH, Sass AM, Rohr JJ, Marshall-Goebel K, Ploutz-Snyder RJ, Ethier CR et al. Automated MRI-based quantification of posterior ocular globe flattening and recovery after long-duration spaceflight. Eye (Lond). 2021 Jul;35(7):1869-1878
- Ferguson CR, Pardon LP, Laurie SS, Young MH, Gibson CR, Brunstetter TJ et al. Incidence and Progression of Chorioretinal Folds During Long-Duration Spaceflight. JAMA Ophthalmology, 2023 Feb 1;141(2):168-175
- Laurie SS, Lee SMC, Macias BR, Patel N, Stern C, Young M et al. Optic Disc Edema and Choroidal Engorgement in Astronauts During Spaceflight and Individuals Exposed to Bed Rest. JAMA Ophthalmology. 2020 Feb 1;138(2):165-172
- Lope-Piedrafita S. Diffusion Tensor Imaging (DTI). Methods in Molecular Biology. 2018;1718:103-116
- Hasan KM, Mwangi B, Keser Z, Riascos R, Sargsyan AE, Kramer LA. Brain Quantitative MRI Metrics in Astronauts as a Unique Professional Group. J Neuroimaging. 2018 May;28(3):256-268
- Greenwald SH, Macias BR, Lee SMC, Marshall-Goebel K, Ebert DJ, Liu JHK et al. Intraocular pressure and choroidal thickness respond differently to lower body negative pressure during spaceflight. Journal of Applied Physiology (1985). 2021 Aug 1;131(2):613-620
- Singh NK, Bezdan D, Checinska Sielaff A, Wheeler K, Mason CE, Venkateswaran K. Multi-drug resistant Enterobacter bugandensis species isolated from the International Space Station and comparative genomic analyses with human pathogenic strains. BMC Microbiology. 2018 Nov 23;18(1):175
- Peng M, Curry SM, Liu Y, Lohawala H, Sharma G, Sharma TP. The ex vivo human translaminar autonomous system to study spaceflight associated neuro-ocular syndrome pathogenesis. NPJ Microgravity. 2022 Oct 28;8(1):44
- Sharma TP, Liu Y, Wordinger RJ, Pang IH, Clark AF. Neuritin 1 promotes retinal ganglion cell survival and axonal regeneration following optic nerve crush. Cell Death Dis. 2015 Feb 26;6(2):e1661
- Richardson, RB. The role of oxygen and the Goldilocks range in the development of cataracts induced by space radiation in US astronauts. Experimental Eye Research, Volume 223, 2022, 109192