Once the digital images have been taken and saved in the screening software, the images then enter the grading pathway and go through a series of grading stages to produce a final outcome grade. This final grade will determine the next stage in the management of any diabetes eye disease detected during the screening process. The pathways within the National Diabetic Eye Screening Programme were discussed in more detail in Part 2 of this three-part series. (See Optician 28.08.05)
The grading scheme
Diabetic eye disease is a progressive condition that goes through a number of changes from its very earliest manifestation to its sight-threatening stages. These changes occur as a continuum but it is possible to study the development of the retinal lesions as the disease process unfolds and start to divide the retinal appearances into a number of different stages, each of which is associated with a risk of progression to sight loss.
There are many different retinal grading schemes depending upon the purpose of the scheme. Examples include very detailed international systems used in research studies like the ETDRS (Early Treatment of Diabetic Retinopathy Study) to simpler and more practical schemes as used in screening programmes. Different national programmes use different schemes and the Scottish programme breaks up the progression stages into more levels than the English programme. In some ways the division into different stages is arbitrary and there will always be cases that sit on the boundary and it can be challenging to decide on which side of the boundary to grade the images. Some cases will obviously sit in the middle of a grade level but some cases are open to interpretation and it is healthy that differences of opinion exist in cases that are borderline.
How the scheme is divided up into grade levels relates to the risk of sight loss associated with the various lesions and also reflects the treatment resources available to manage the diabetic eye disease. The point of referral may vary in different countries depending upon the availability of ophthalmologists and access to treatment options such as laser. As evidence and data from diabetic eye screening programmes increases (some programmes in the UK have now been running over 10 years and have significant data on progression in a normal population as opposed to within the research sample used in studies like ETDRS) the grading schemes can be refined and there have been some recent changes to the retinal lesions associated with each level of retinopathy in the English national programme. Some definitions have been refined to give greater discrimination between observable and referable lesions.1
This article will discuss the current grading scheme being used in England.
Grading an image
It is important to approach grading an image systematically, particularly if you are grading a series of images over a period of time to avoid visual fatigue and ‘zoning out’. Grading is essentially an image recognition task and knowing the lesions, how they appear and how they vary with disease progression is essential to be able to interpret an image. As optometrists we know that our perception fills in any gaps in the areas we are not looking at so it is not enough to just look at an image. A systematic study of the image so that all parts are examined, for example starting with the disc and following the major vessels, helps to ensure that no lesions are missed.
The grading software includes various image manipulation tools that help to highlight lesions. For example ‘red free’ can pinpoint a small microaneurysm much more quickly than trying to locate a small red spot against a red/orange background. There are also contrast enhancement tools, zoom and magnification tools available. Beware of artefacts on the image. Most cameras appear to have various spots that are visible on the final images. These will always appear in the same place relative to the image boundary and that helps to avoid grading them as retinal lesions.
The level of retinopathy is determined within the software using a ‘features-based’ approach. The grader identifies the various lesions present and selecting this feature produces a grade as determined by rules applied within the software. It is important that lesions are only recorded if they are definitely present so for example using both colour and red-free images helps to distinguish between a pigment spot versus a blot haemorrhage.
Image quality
Image quality will vary within the range of patients seen for eye screening. It is affected by a range of factors including media opacities, pupil dilation and patient mobility.
There are definitions that enable a grader to decide whether an image can be safely graded. An image is now considered to be either ‘adequate’ or ‘inadequate’.
Photographers must capture two nominal 45º fields per eye (one fovea centred and one disc centred). A combined assessment of field position and image quality should be made for each eye. Images must be graded for diabetic eye disease only if the grader is confident the quality is sufficient. All grading must be performed by trained qualified staff (City & Guilds Certificate).
The definition of adequate is that both the centre of the fovea or the complete optic disc must be greater than two disc diameters (DD) from the edge of the image and the fine vessels must be visible within one DD of the centre of the fovea or on the surface of the disc. It is now possible for a screener to take a series of retinal images and for the grader to use a ‘jigsaw’ approach to ensure that the combined view is equivalent to the normal adequate fovea and disc centred approach.
An important qualification to this is that if sight-threatening diabetic retinopathy (STDR) can be detected on any of the images the quality should be considered as adequate and the patient referred to ophthalmology. This means that poor quality images should be studied especially carefully to ensure that no sight threatening lesions are visible. An important example of this is not to assume that a very hazy image is the result of cataract as there is a possibility that the haze could be caused by a vitreous haemorrhage. See Table 1 for a summary of grading levels.
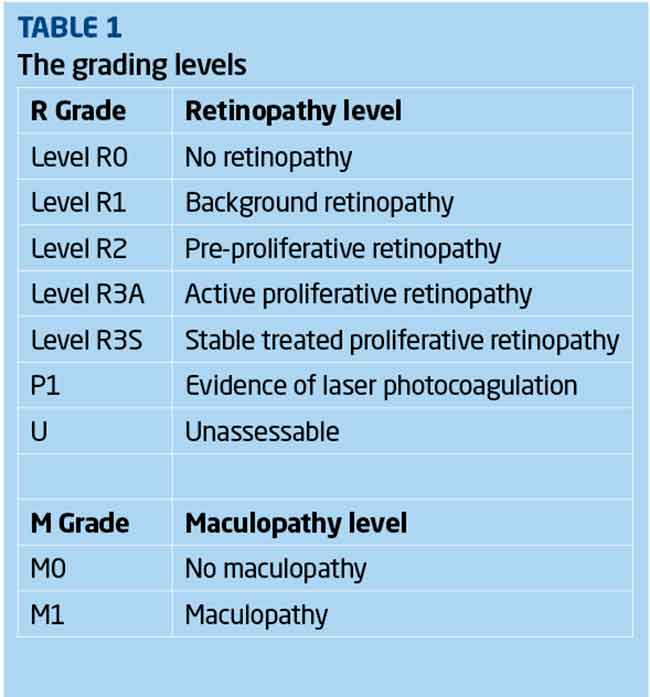 Normal R0
Normal R0
An image with no evidence of any lesions associated with diabetic retinopathy should be graded R0. However, other lesions which may or may not be sight threatening may be detected and should be referred according to local protocols. Some retinal appearances can ‘mimic’ some diabetic retinopathy lesions and it is important to be able to distinguish between features such as a pale spot being either a drusen or an exudate (particularly as some drusen are quite reflective) or myelinated nerve fibres appearing very similar to cotton wool spots (especially if they are not adjacent to the optic disc). This is the stage at which patients should be encouraged to manage their diabetes as well as they possibly can. Evidence has shown that there is a glycaemic memory that affects disease progression so that a past period of poor diabetes control can influence progression at a future date.
Background R1
[CaptionComponent="2959"]
The earliest stage of visible diabetic retinopathy is graded R1 and is labelled ‘background retinopathy’. This is an indication that there are microvascular changes present within the retina and optimal control of blood glucose and blood pressure are the primary management strategies used by the GP or diabetes specialist responsible for the patient’s diabetes.
The main lesions associated with this level are summarised in Table 2.

Background diabetic retinopathy is not in itself sight-threatening and does not require referral to ophthalmology. It is, however, an indicator of early microvascular disease and patients should be advised to look at their diabetes and blood pressure control. Management is annual recall to diabetic eye screening.
[CaptionComponent="2960"]
A note of caution: all these features may also be present in sight-threatening retinopathy, so a careful study of the retinal images is important, especially as the number of these lesions increases.
Pre-proliferative R2
[CaptionComponent="2961"]
This is a clinically identifiable stage of retinopathy that precedes and to some extent predicts proliferative retinal changes. It is graded R2 and labelled pre-proliferative retinopathy. The main features that classify this level of retinopathy are increasing signs of retinal ischaemia and the vascular changes that accompany this. Progressive endothelial cell loss in the capillaries causes occlusion within the capillary network resulting in areas of chronic retinal ischaemia. This can progress quite quickly to proliferative retinopathy if not properly managed.
[CaptionComponent="2962"]
The main lesions associated with this level are summarised in Table 3.

If an image is determined to be an R2 grade then the patient should be referred to see an ophthalmologist within 13 weeks of the final outcome grade. If the diagnosis is confirmed then management is generally medical. Regular follow-ups within ophthalmology are usual. Aggressive management of blood pressure is important but care must be exercised in tightening control of the blood glucose levels, as too rapid an approach can result in a worsening of the retinopathy that may then progress to the proliferative stage. A steady approach over many weeks/a small number of months is often the preferred management plan.
Active proliferative R3A
[CaptionComponent="2963"]
The recent changes to the grading scheme have resulted in two categories for R3. R3A indicates that the proliferative changes are active and require management. R3S indicates the phase after treatment for R3A when the retinal condition is considered to be stable (see next section).
[CaptionComponent="2964"]
The definitive feature of the proliferative phase of diabetic retinopathy R3A is new vessels. These are immature vessels that develop as a result of retinal ischaemia. They can grow on the disc (NVD), elsewhere on the surface of the retina (NVE) and on the iris (rubeosis). They are mediated by the release of vascular endothelial growth factor (VEGF) within the retina and this release is stimulated by hypoxic retinal tissue. New vessels are presumed to be an attempt (doomed to failure) at revascularisation of the ischaemic areas of retina. Unlike collateral vessels which redirect venous flow within the retina, new vessels have a random appearance with no obvious purpose to the direction they grow in. They typically grow from the venous circulation, so particular attention should be paid to inspecting the retinal veins across the whole image. They have circular frond-like tips and grow in the vitreo-retinal interface with no support from the surrounding tissue. The vessel walls are thus fragile and may rupture
causing pre-retinal and vitreous haemorrhages. New vessels growing in the anterior chamber angle lead to intractable rubeotic glaucoma.
Sometimes a grader will find that one eye shows proliferative retinopathy with little or no retinopathy in the other eye. This is highly indicative of a compromise to the retinal circulation in one eye and may indicate a systemic condition such as carotid insufficiency on that side of the head rather than as a result of poorly controlled diabetes.
The features classifying R3A are summarised in Table 4.

Proliferative retinal changes require urgent referral to ophthalmology. Cases should be referred within two weeks of the initial screening encounter and should be seen in the Hospital Eye Service (HES) within two weeks of being referred. Image triage within the screening pathway allows for rapid identification of potential R3A allowing for priority grading and fast-track referral. There are a range of management options now available to ophthalmologists managing proliferative retinopathy including pan-retinal photocoagulation but discussion of this is beyond the scope of this article and will instead be covered in a future CET article.
Stable treated proliferative retinopathy R3S
[CaptionComponent="2965"]
Stable treated proliferative retinopathy R3S is defined as retinal images with evidence of peripheral retinal laser treatment and with stable retina with respect to reference images taken at or within three months after discharge from ophthalmology. These patients are then reviewed within the digital surveillance pathway.
A referral outcome grader will always be responsible for the decision as to whether the images indicate a stable retina. That decision is based on a combination of digital images and patient history. If there is any doubt, then the images should be graded R3A and the patient referred for an urgent review by an ophthalmologist. If there are no reference images available from ophthalmology, either upon discharge or soon after, then it may be necessary to re-refer the patient to acquire this essential benchmark visual data.
The split into R3A and R3S grades allows for urgent attention where proliferative disease is active and a robust monitoring pathway outside the hospital eye service for discharged patients once treatment has allowed the condition to stabilise with the potential for rapid re-referral should reactivation of proliferative eye disease occur.
An R3S grade is only valid if there are no significant changes from the baseline discharge images. These features are summarised in Table 5.

No maculopathy M0
Maculopathy is defined in terms of the lesions evident within the macular region and visual acuity is a factor in making the diagnosis. In the absence of any of the defined markers for diabetic maculopathy (see section M1), the image is graded M0, even if there is background diabetic retinopathy present in the macula (Figure 7).
Maculopathy M1
The English National Diabetic Eye Screening Programme defines the macula as that part of the retina which lies within a circle centred on the centre of the fovea whose radius is the distance between the centre of the fovea and the temporal margin of the disc. It is effectively the area of retina lying between the vascular arcades.
Although proliferative retinopathy can lead to severe sight loss, the most common cause of significant sight loss in diabetic eye disease is diabetic maculopathy because this is the region of the retina responsible for good visual acuity and colour vision. Ophthalmologists are interested in identifying patients with clinically significant macular oedema (CSMO) as those requiring treatment because it is this oedema that disrupts the foveal receptors and affects vision.
CSMO is defined by the ETDRS (Early Treatment of Diabetic Retinopathy Study) as any of the following retinal features:
- Thickening of the retina at or within 500 microns of the centre of the macula
- Hard exudates at or within 500 microns of the centre of the macula (Figure 8), if associated with thickening of the adjacent retina (no residual hard exudates remaining after the disappearance of retinal thickening)
[CaptionComponent="2966"]
- A zone or zones of retinal thickening one disc area or larger, any part of which is within one disc diameter of the centre of the macula.
CSMO is by definition a thickening of the retina at the macula and consequently it is thus best seen with stereoscopic techniques such as slit lamp biomicroscopy with Volk lens. More recently the use of OCT giving a cross-sectional view of the macula allows regions of fluid accumulation to be easily seen.
Clinically significant macular oedema cannot be overtly detected in 2D views such as the digital photographic images used in the screening programme. To be able to grade diabetic maculopathy from digital images requires the use of surrogate markers which are macular changes that strongly correlate to the presence of macular oedema. These surrogate markers do not guarantee the presence of macular oedema and images showing signs of visible diabetic retinopathy within the macular region may or may not have clinically significant macular oedema present.
The surrogate markers currently used in this grading scheme are summarised in Table 6.

The definition of a group of exudates has now been classified as follows: ‘a group of exudates is an area of exudates that is greater than or equal to half the disc area and this area (of greater than or equal half the disc area) is all within the macular area.’ (Figure 9).
[CaptionComponent="2967"]
In order to ascertain the area of exudates, the outer points of the exudates are joined and this enclosed area compared to half the area of the optic disc. Reference images have been provided and can be accessed at: www.gov.uk/government/uploads/system/uploads/attachment_data/file/402294/Revised_Grading_Definitions_V1_3_1Nov12_SSG.pdf
Visual acuity is a crucial element in deciding if the presence of microaneurysms or haemorrhages within one DD of the foveal centre can be considered a marker for maculopathy. If the cause of the reduced visual acuity (6/12 or worse) is known and is not diabetic macular oedema then the image is graded M0 and not M1.
Maculopathy cases should be referred and should be seen by ophthalmology within 13 weeks of the final outcome grade.
Laser photocoagulation P1 (Figure 7)
If there is evidence of previous photocoagulation including focal or grid macular laser or peripheral pan-retinal photocoagulation then a ‘P’ grade is also allocated. Evidence of previous laser is graded P1.
Unassessable images U
As discussed earlier in this article some images will not meet the criteria for ‘adequate to grade’ after first studying them carefully for any evidence of referable retinopathy. These images are assessed by a referral outcome grader. In some cases the poor image quality may have been a technical issue and the patient should be recalled for a further digital imaging session as soon as possible. If the poor image quality is more ‘organic’ and relates to the quality of the ocular media, or persistent poor dilation (as sometimes happens following cataract surgery or in eyes with a dark iris) or poor mobility resulting in difficulty getting some or any digital images, then the patient should be graded ‘U’ and recalled to a slit-lamp clinic. If the screening programme has a policy of obtaining anterior eye images in such cases, these can help in deciding the cause of the poor quality image. Arrangements for the provider of slit-lamp clinics to the eye screening programme may differ between programmes depending upon how the service has been commissioned. Patients must be seen within 14 weeks of the final outcome grade.
Conclusion
Diabetic eye disease is a progressive condition that if it is not managed appropriately, either in the early stages by good management of the blood glucose levels and blood pressure or in the later stages by good attendance at HES appointments can then lead to severe sight loss. As discussed in Part 2 of this series (Optician 28.08.15) there is now a national screening programme set up to monitor all patients with diabetes over the age of 12 years. Because there are early signs of overt diabetic eye disease and because these signs can be detected by the screening programme it is possible to catch the disease process at an early, more manageable, stage. There is little reason for anyone to go blind these days as a result of diabetic eye disease. Quality grading of the retinal images according to the national programme protocols discussed above allows for classification of patients according to the severity of the diabetic retinopathy. Appropriate management pathways can be initiated to give patients the best chance of reducing the potentially devastating consequences of sight loss as a result of their diabetes.
Read more
A practitioner’s perspective: Diabetic retinopathy screening
Diabetes part 1 – disease overview
Diabetic retinopathy VRICS – part 2
References
1 Diabetic Eye Screening Revised Grading Definitions Version 1.3, 1 November 2012.
2 Venous loops and reduplications in diabetic retinopathy Prevalence, distribution, and pattern of development – Toke Bek Department of Ophthalmology, Århus University Hospital, DK-8000 Århus C, Denmark.
Peter Mitchell is clinical manager and senior optometrist, London North East DESP