
The following cases raise a number of points of interest:
- All images and video were taken using a smartphone (in this case, the iPhone 11) and a slit-lamp adaptor. The resolution of modern smart phone cameras is easily good enough to capture useful clinical signs as either stills or short videos
- The magnification of the slit-lamp may be complemented by that of the image on the phone either during capture or post-capture. Post-capture images may be further enhanced (for example, filters added or contrast enhanced) by image software included in standard software platforms.
- Since the initial lockdown, there has been restricted access to many health care services, for example a GP, and eye care professionals are seeing an increase in the numbers reporting problems such as those seen here that can be dealt with by available ECPs.
- Use of image capture equipment as shown here can help to reduce the duration of time spent in close proximity to a patient at the slit-lamp. The viewing screen on the smart phone can be seen from some distance and capture may be set to operate by voice command or by a Bluetooth-linked remote-control button (as is supplied, for example, with the slit-lamp adaptor provided by Bond-Eye). Also, video capture can be viewed and measurements taken away from the patient and using accurate digital timings.
- It is essential to use the slit-lamp orange absorption filter (Wratten) along with the blue excitation filter to achieve the best image of any stain or fluorescence (figure 1).
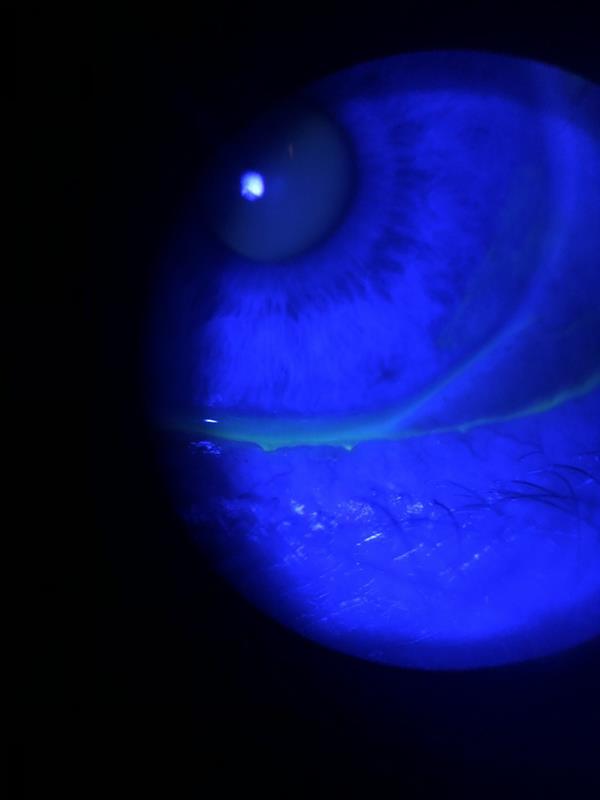 Figure 1a: Image of an eye under blue light after fluorescein instillation.
Figure 1a: Image of an eye under blue light after fluorescein instillation.
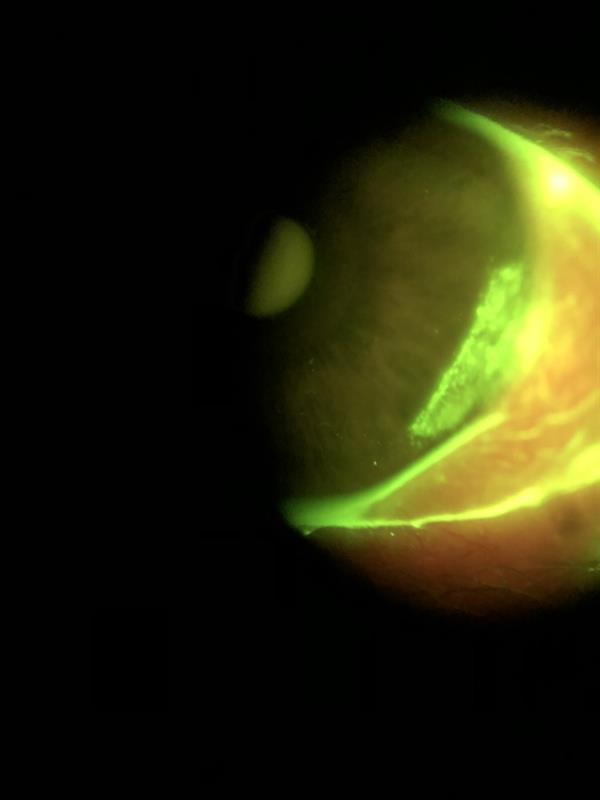 Figure 1b: Same eye with introduction of Wratten filter revealing peripheral corneal epithelial damage (Images: Beth Ralph)
Figure 1b: Same eye with introduction of Wratten filter revealing peripheral corneal epithelial damage (Images: Beth Ralph)
Case 1
Patient booked in to the dry eye clinic.
Presentation
- Female age 61
- Reason for contact; had contacted GP at beginning of lockdown due to uncomfortable eyes. Had been recommended drops (name not known). Little used as ‘did not like them’.
- Working from home due to Covid lockdown. Uses laptop seven to eight hours per day. Renovating property ready to move into – likely exposure to dust.
- General health; menopausal, reports hot flushes for last seven to eight years. Asthma.
- Medications; salbutamol inhaler as required.
- History; seasonal allergic rhinitis but reports no symptoms at present.
- CL wear; previous soft lens wear, lapsed c20 years ago due to poor comfort.
Clinical findings
- Eyes still ‘uncomfortable,’ R worse than left
- Refraction
- R; -3.50 (6/6 +2)
- L; -4.00 (6/6 +2)
- Add + 2.00 (N5 R&L)
- Slit-lamp with fluorescein
- Left (figure 2); complete blink, line of inferior desiccation stain, scattered temporal punctate stain, fluorescein break-up time five seconds
- Right (figure 3); incomplete blink, band of inferior desiccation stain, scattered temporal punctate stain, fluorescein break-up time four seconds
- Slit-lamp with white light (figure 4)
- Blepharitis crusting around lashes, R; grade 2, L; grade 1
- Inspissation of meibomian gland openings, R>L
Figure 2: Video of fluorescein break-up time for left eye. At three seconds inferior desiccation visible, at five seconds break up spots visible
Figure 3: Video of fluorescein break-up time for right eye. Pre-blink appearance shows multiple sites of break-up, greater inferior desiccation than left and scattered desiccation stain over cornea. Moment of maximum blink showing clear lagophthalmos
Figure 4a: Right lower lid showing crusting of the lashes, irregular lid margin and whiteness of meibomian gland orifices due to inspissation.
Figure 4b: Upper lid lash crusting
Note; after further questioning to ascertain possible cause of R>L asymmetry of signs, patient revealed she is aware of rubbing the right eye more than the left, and prefers to sleep on her right side. Video capture confirmed that the lagophthalmos is only apparent on the right
Management
- Lid therapy; twice daily use of a warm compress (issued with Eye Doctor mask) followed by lid massage
- Eye lid cleaning; Blephasol Duo and pads to cleanse lids after lid heating and massage
- Tears; Theoloz Duo gel (twice a day) or Theoloz Duo drops (every four hours) discussed. After previous experience and in-practice trial, patient preferred gel option.
- Information given about safe computer use and blinking
- Review booked for 1 month.
Case 2
Patient booked in to the dry eye clinic.
Presentation
- Female age 50
- Patient working from home, desktop computer use six hours a day
- Reason for visit; full time soft contact lens wearer but ceased wear ‘recently’ due to discomfort
- History; had been referred to hospital eye service pre-lockdown due to a suspected ocular allergy. HES confirmed blepharitis and dry eye and ordered an allergy test. Allergy test had been postponed due to lockdown. Allergy symptoms now resolved and patients wants to resume contact lens wear but eyes still feel uncomfortable
- General Health; menopausal
- Medications;
- otc antihistamine (oral, one a day)
- Hyloforte (preservative-free, sodium hyaluronate 2 mg/mL) used twice a day
- Uses warm compress ‘three times a week’
- Ocular history; previous full time wear of Clariti 1-day soft lenses. No spectacles worn for at least two years as ‘very out if date’. These were supplied today to a new prescription.
Clinical findings
- Eyes ‘generally uncomfortable’
- Refraction;
- R; +2.00 / -0.25 x 110 (6/6)
- L; +2.00 / -0.50 x 100 (6/6)
- Add; +1.75 (N5 R&L)
- Slit-lamp and fluorescein (figure 5); break up time three seconds and low-grade epithelial staining R&L
Figure 5 left: Patches of tear break up after three seconds
Figure 5 right: Patches of tear break up after three seconds
Management
- Increase heat compress to twice daily and introduce post-heat massage and lid cleansing (Blephasol Duo)
- Increase frequency of drop use as symptoms require
- Advice on computer use given
- Advice on contact lens wear resumption after next review in two weeks.
Beth Ralph is a contact lens optician & consultant based at Bird Opticians in Sheffield.