Angioid streaks represent breaks in Bruch's membrane - the transparent, inner layer of the choroid situated adjacent to the retinal pigment epithelium.  In patients with angioid streaks, the membrane is abnormally thickened, calcified and fragile. Approximately half of cases are idiopathic, and half occur in association with systemic disease:
In patients with angioid streaks, the membrane is abnormally thickened, calcified and fragile. Approximately half of cases are idiopathic, and half occur in association with systemic disease:
Pseudoxanthoma elasticum (most common) - an inherited connective tissue disorder. Approximately 85 per cent of patients with pseudoxanthoma elasticum have angioid streaks. Patients develop loose skin ('chicken skin') and accelerated atherosclerosis, and have an increased risk of gastrointestinal bleeding
Paget's disease - a chronic, progressive disease resulting in abnormal, deformed, thickened and brittle bones. Features include bone pain, bowing of the legs, pathological fractures, hearing loss, enlargement of the skull and congestive cardiac failure. (Optic atrophy is a rare complication of Paget's disease, due to bony compression of the optic canal)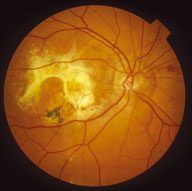 Less common causes - other connective tissue disorders (such as Ehlers-Danlos syndrome and Marfan syndrome), haemoglobinopathies (for example, sickle cell disease), acromegaly and lead poisoning.
Less common causes - other connective tissue disorders (such as Ehlers-Danlos syndrome and Marfan syndrome), haemoglobinopathies (for example, sickle cell disease), acromegaly and lead poisoning.
Register now to continue reading
Thank you for visiting Optician Online. Register now to access up to 10 news and opinion articles a month.
Register
Already have an account? Sign in here